
Learn what causes flat feet, common symptoms to watch for, and the most effective exercises, footwear, and treatment options for reducing pain and improving foot function.
You probably discovered it by accident. A wet footprint on the poolside, a silhouette in the sand, a throwaway comment from a doctor during a routine exam. Your arch isn't there — or barely is. And now you're wondering how long it's been missing.
Flat feet, also called fallen arches, are one of the most common structural variations in the human foot. Research suggests that roughly 20 to 30 percent of adults have some degree of flatfoot, and the majority of them never experience a single symptom. For others, flat feet are the undiagnosed reason behind years of arch pain, knee trouble, lower back fatigue, and shoes that wear out unevenly on one side.
The difference between those two groups isn't luck. It comes down to the type of flat foot you have, the strength and mobility of the structures around it, and whether your footwear is helping or quietly making things worse.
This guide breaks all of that down in plain language — what flat feet actually are, what causes them, whether yours are worth treating, and what the evidence says about what works.
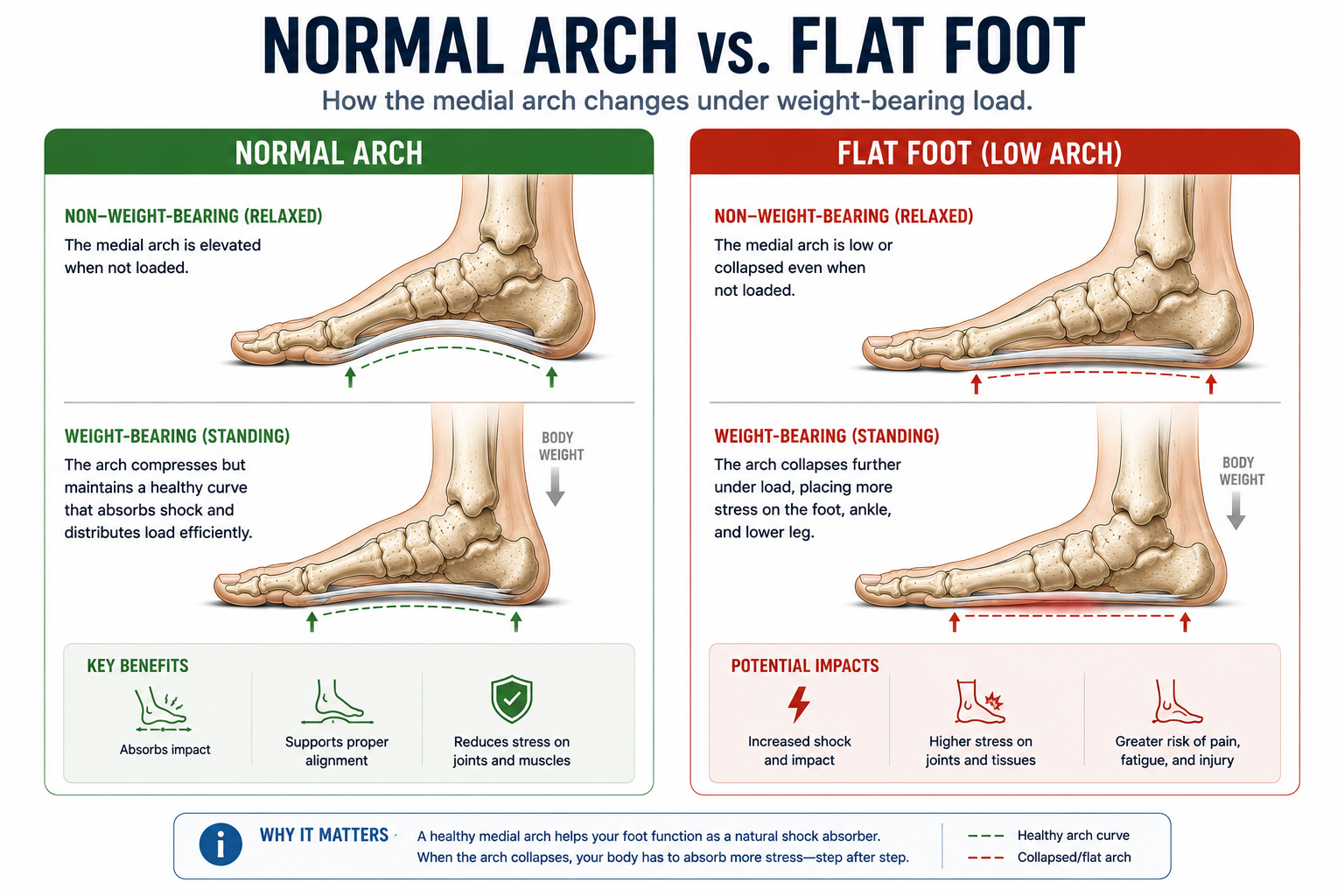
What are flat feet?Flat feet occur when the medial longitudinal arch — the inward curve along the inner edge of the foot — is significantly reduced or absent during weight-bearing. Instead of rising off the ground when you stand, the arch collapses, bringing the inner foot closer to or flush with the floor. This changes how load is distributed across the foot and can alter mechanics all the way up the leg.
Featured Snippet: What Are Flat Feet?Flat feet occur when the arch on the inside of the foot collapses or fails to develop fully. In some people this causes no symptoms, while others experience foot pain, heel pain, ankle instability, knee discomfort, or fatigue during walking and standing. Flat feet are extremely common, affecting roughly 20–30% of adults.
Common Signs of Flat Feet
✓ Little or no visible arch when standing
✓ Foot and arch fatigue during the day
✓ Heel pain, especially after long periods on your feet
✓ Arch pain or burning along the inner foot
✓ Shoes wear down unevenly on the inner edge
✓ Ankles that roll inward when standing
✓ Knee discomfort without an obvious injury
✓ Lower back or hip fatigue that worsens with standing
To understand flat feet, it helps to understand what the arch is actually doing in a healthy foot.
The medial longitudinal arch is the curved, inward-facing structure that runs along the inner edge of your foot from heel to the base of the big toe. Think of it like the arch of a stone bridge: it's not decorative. It's structural. The arch distributes your body weight across the foot, absorbs the shock of each step, stores elastic energy during loading, and releases it during push-off. Without it, the foot loses both its shock-absorbing capacity and its mechanical efficiency.
In a flat foot, this arch is significantly lower than normal during weight-bearing. The plantar fascia, the intrinsic muscles of the foot, and several key tendons — particularly the posterior tibial tendon — are all responsible for maintaining arch height. When any combination of these structures is compromised, loose, or weak, the arch collapses.
Most flat feet fall into one of two categories: present from birth (congenital) or developed over time (acquired). We'll cover both in the next section.
Key Takeaway: A flat foot isn't simply a missing arch. It's a sign that the structural and muscular system that holds the arch in place is under stress, overloaded, or weakened. Understanding which factor is driving it determines what actually helps.
Flat feet rarely have a single cause. In most adults, they develop through a combination of factors that accumulate over years.
Some people are simply born with flat feet, or with a foot structure that's predisposed to arch collapse. Infants always appear flat-footed because the arch doesn't fully develop until early childhood, typically between ages 3 and 6 as the foot's ligaments tighten and the intrinsic muscles mature. For some children, that developmental process doesn't complete fully, and the flat foot persists into adulthood.
Joint hypermobility, where the connective tissues throughout the body are looser than normal, is one of the most common underlying contributors to flat feet. When the ligaments that support the arch are overly lax, they allow the arch to collapse under bodyweight even when muscle strength is adequate. People with hypermobility-related flat feet often have flexible joints throughout the body, not just in the foot.
The structures that hold the arch up are subject to decades of cumulative loading. As people age, the plantar fascia loses some of its elasticity, ligaments gradually lengthen, and the intrinsic foot muscles weaken — particularly in people whose footwear has done the structural work for them for years. What starts as a moderate arch in your thirties can become a significantly flatter one by your fifties.
This is the most common cause of adult-acquired flatfoot, and it's significantly underdiagnosed. The posterior tibial tendon runs along the inner ankle and is the primary active support structure for the arch. When this tendon becomes inflamed, degenerates, or tears — often from repetitive stress or overuse — the arch progressively collapses on the affected side.
A hallmark sign of posterior tibial tendon dysfunction is a flat foot that develops on only one side. If your flat feet are asymmetrical and the inner ankle is tender, this warrants professional evaluation.
A fracture or ligament injury in the midfoot or ankle can disrupt the arch mechanics permanently if the structures don't heal in their correct alignment. Lisfranc injuries (midfoot sprains or fractures) are particularly associated with arch collapse.
Body weight is a direct variable in arch loading. A systematic review published in the Journal of the American Podiatric Medical Association found that higher body mass index is significantly associated with flatfoot prevalence in adults. Increased load over time compresses and eventually overcomes the structural integrity of the arch, particularly when combined with other risk factors like ligament laxity or weak intrinsic muscles.
Flat feet are asymptomatic for many people. But when symptoms do develop, they tend to follow recognizable patterns.
Aching, burning, or soreness along the inner arch of the foot, especially during or after activity.
Generalized discomfort under the heel that may overlap with plantar fasciitis symptoms.
Fatigue, tenderness, or aching along the inside of the ankle, particularly after standing or walking.
Discomfort on the inner side of the knee caused by changes in foot and leg alignment.
Tired, heavy, or overworked calves and shins after moderate activity.
Mild swelling around the arch or inner ankle, especially after prolonged standing.
Feet tire quickly during long periods of standing, even on cushioned or supportive surfaces.
Shoes wear down faster on the inner heel and forefoot than on the outer edge.
Why do symptoms vary so much between people? Two factors matter most. First, the degree of arch collapse: a mildly flat foot places meaningfully less strain on surrounding structures than a severely collapsed one. Second, the compensatory capacity of the surrounding muscles. A person with flat feet and strong, well-conditioned foot and ankle muscles can often offset the mechanical disadvantage entirely. Symptoms tend to emerge when the flat foot exceeds what the surrounding musculature can compensate for.
Run through this quickly. Check any that apply:
If two or more of these apply, flat feet are likely contributing to your symptoms. This isn't a clinical diagnosis, but it's a meaningful starting point for understanding what to look for and what to discuss with a professional.
This distinction is one of the most important in flatfoot evaluation, and it determines much of the treatment direction.
The arch appears normal when sitting or when weight is removed from the foot, but collapses when standing. This is the most common type of flat foot and is often associated with ligament laxity, hypermobility, or weak foot muscles.
Arch at Rest (Sitting)
Arch appears normally.
Arch When Standing
Arch collapses under body weight.
Arch on Tiptoe
Arch typically reappears.
Prevalence
More common than rigid flat feet.
Common Age of Onset
Often present from childhood or develops gradually in young adulthood.
Typical Causes
Ligament laxity, hypermobility, muscle weakness, or inherited foot structure.
Pain Level
Often mild or absent, though symptoms may develop with prolonged standing or activity.
Treatment Approach
Usually responds well to strengthening exercises, supportive footwear, and orthotics when needed.
The arch remains collapsed regardless of whether weight is applied to the foot. This type is less common and often has a structural cause that requires professional evaluation.
Arch at Rest (Sitting)
Arch remains collapsed.
Arch When Standing
Arch remains collapsed.
Arch on Tiptoe
Arch does not reappear.
Prevalence
Less common than flexible flat feet.
Common Age of Onset
Can occur at any age and is often acquired over time.
Typical Causes
Tarsal coalition, arthritis, posterior tibial tendon dysfunction (PTTD), or other structural abnormalities.
Pain Level
More frequently associated with pain, stiffness, and functional limitations.
Treatment Approach
Often requires professional assessment and may involve orthotics, physical therapy, imaging, or other medical interventions.
Flexible flat feet are by far the more common presentation. Because the arch returns when weight is removed, the supporting muscles and ligaments are still functional — they're just not managing the load during standing and walking as efficiently as they could. This is the type most responsive to conservative treatment: targeted strengthening, appropriate footwear, and orthotics when needed.
Rigid flat feet are a different clinical picture. When the arch remains collapsed regardless of weight-bearing status, the cause is often structural: a tarsal coalition (two or more foot bones fused together), significant arthritis, or a posterior tibial tendon that has torn rather than just degenerated. Rigid flat feet are more consistently painful, more functionally limiting, and more frequently require imaging and professional intervention.

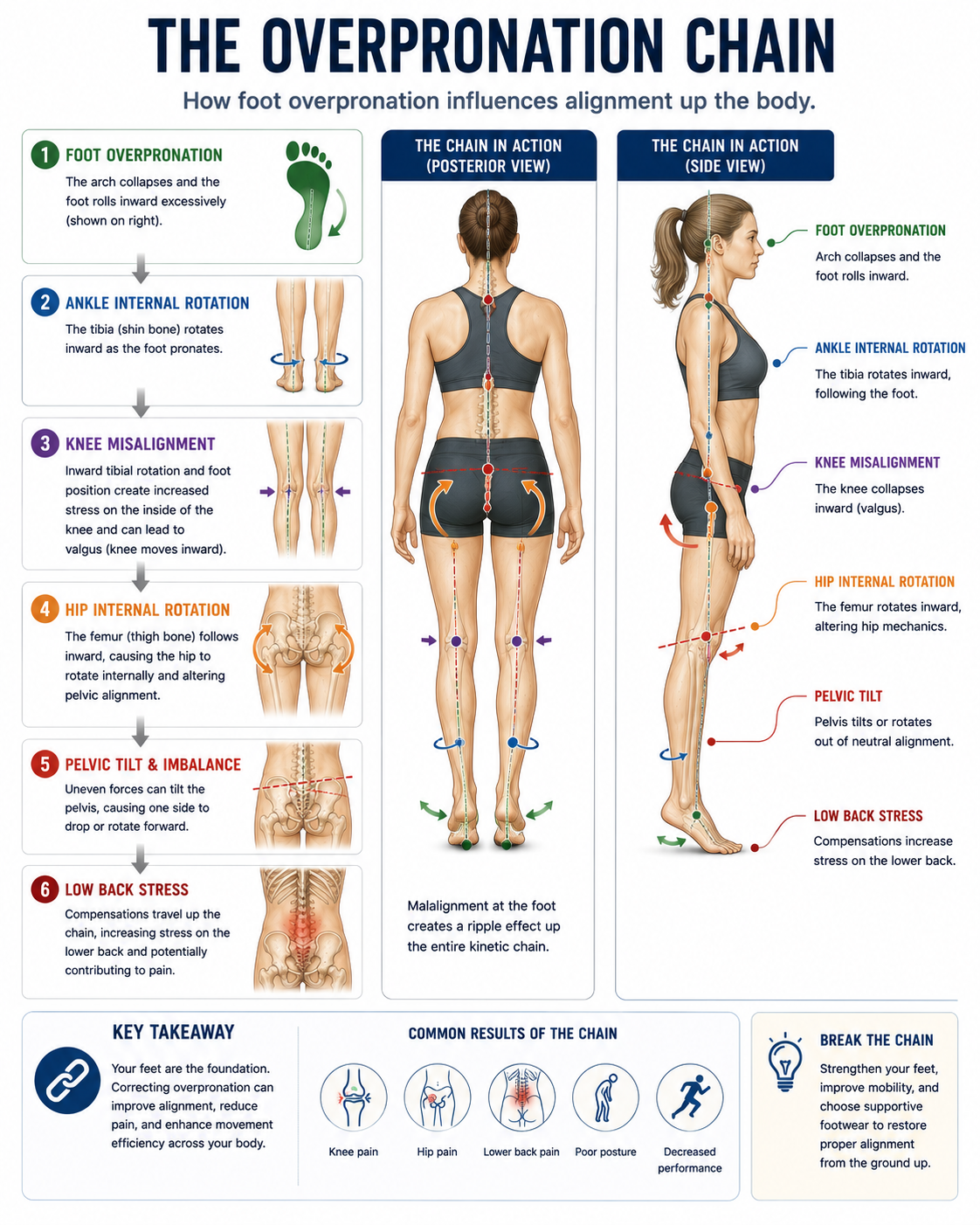
The foot is the foundation of the body's weight-bearing chain. When the foundation is misaligned, the effects can travel upward.
Plantar Fasciitis
The plantar fascia, the thick connective tissue band that spans the arch, is placed under greater repetitive tension when the arch collapses with each step. This is one of the reasons flat feet are a well-established risk factor for plantar fasciitis. → See What Is Plantar Fasciitis?
Achilles Tendon Pain
Overpronation caused by flat feet rotates the heel bone inward, which alters the alignment of the Achilles tendon. This creates asymmetrical loading in the tendon over thousands of steps per day, increasing injury risk.
Shin Splints
The posterior tibialis muscle works harder in people with flat feet because it's trying to dynamically support an arch that isn't getting enough passive help. That chronic overload manifests as medial tibial stress syndrome — commonly called shin splints — particularly in runners and people who increase their activity levels rapidly.
Knee Pain
Excessive inward rolling of the foot during the gait cycle rotates the tibia internally, which places stress on the medial compartment of the knee. Research published in Clinical Biomechanics has documented the correlation between overpronation and increased knee adduction moments, a known contributor to medial knee pain. → See Overpronation Explained
Hip and Lower Back Discomfort
This is where many people are most surprised. Because the leg's rotation pattern is altered by foot mechanics, the effects can travel all the way to the hip and lumbar spine. People with longstanding flat feet and overpronation occasionally report chronic low back pain that improves meaningfully once their foot alignment is addressed — not because the spine was the problem, but because the problem started at the floor.
Bunions
A bunion is a bony prominence that forms at the base of the big toe joint, and flat feet are one of the most consistent contributing factors. When the arch collapses and the foot pronates excessively, load is redirected through the inner forefoot with each push-off. Over time, this altered force pattern pushes the big toe toward the lesser toes, gradually deforming the first metatarsophalangeal joint. People with flat feet tend to develop bunions earlier and more severely than those with neutral or high arches.
Metatarsalgia
Metatarsalgia is pain and inflammation in the ball of the foot, and it's a predictable downstream consequence of arch collapse. When the arch flattens, the metatarsal heads — the five long bones that form the ball of the foot — are forced to absorb a disproportionate share of impact load that a healthy arch would otherwise distribute. The result is forefoot overload: a burning, aching, or bruised sensation across the ball of the foot that worsens with walking or standing and improves with rest. → See Foot Pain Location Guide
This is the question most people are actually asking, and it deserves an honest answer.
For structural flat feet — where the arch is genuinely low due to bone shape, fused joints, or significant tendon damage — the architecture of the foot cannot be meaningfully changed through exercise or footwear alone. The foot's bony structure is what it is.
But for the majority of adults with flexible flat feet, the picture is more nuanced and more hopeful. Research has shown that targeted intrinsic foot muscle training can meaningfully increase the height of the medial arch during standing and walking. A study published in the Journal of Electromyography and Kinesiology found that eight weeks of progressive short foot exercise training produced measurable increases in navicular height — the most commonly used clinical measure of arch height.
The more important question may not be whether the arch itself can be "fixed," but whether the pain and functional limitations that come with flat feet can be resolved. For many people, the answer to that is yes — even when arch height doesn't change significantly. The goal of treatment is function, not a perfect arch silhouette.
What can realistically improve:
What typically doesn't change through conservative treatment alone:
Exercises don't work for flat feet by simply "building the arch." They work by strengthening the muscles that actively support the arch during loading — primarily the intrinsic foot muscles and the posterior tibialis. Here are the five with the strongest evidence base.
Purpose: Directly activates the abductor hallucis and flexor digitorum brevis — the two primary intrinsic muscles responsible for maintaining medial arch height.
How To Perform:
Sit in a chair with your foot flat on the floor, all toes relaxed. Without curling your toes, attempt to shorten the foot by drawing the ball of your foot toward your heel. You should feel the arch dome upward. Do not let the toes curl or grip the floor.
Sets/Reps: 3 sets of 10 holds (5–10 seconds each), per foot
Common Mistakes: Gripping the toes instead of shortening the foot; allowing the heel to lift; performing the movement too quickly. This exercise is deceptively hard at first. Most people's intrinsic foot muscles are undertrained.
.png)
Purpose: Develops independent motor control of the big toe and the lesser toes, which is essential for dynamic arch stability during walking.
How To Perform:
Place your foot flat on the floor. First, lift only your big toe while keeping the other four toes down. Hold 5 seconds, then lower it. Next, press the big toe down while lifting only the lesser four toes. Alternate back and forth.
Sets/Reps: 3 sets of 10 alternations per foot
Common Mistakes: Moving the ankle instead of the toes; using the foot as one unit rather than separating the movements. This takes practice. Expect it to feel nearly impossible the first time.
Purpose: Strengthens the gastrocnemius, soleus, and posterior tibialis — all of which contribute to dynamic arch support during the push-off phase of walking.
How To PerformS
tand with feet hip-width apart. Rise slowly onto the balls of your feet, hold 2 seconds at the top, then lower slowly. Progress to single-leg heel raises as strength improves.
Sets/Reps: 3 sets of 15 double-leg; work toward 3 sets of 10 single-leg
Common Mistakes: Rising too quickly; letting the ankles roll outward at the top; not completing full range of motion through the heel lowering phase.
Purpose: Tight calf muscles restrict ankle dorsiflexion, which increases the mechanical load on the arch during gait. This is directly relevant to flat feet, where the arch is already under greater strain. → See How Tight Calves Cause Foot Pain
How To Perform:Stand facing a wall. Place one foot back with the knee straight and press the heel firmly into the floor. Lean forward until you feel the stretch in the back of the lower leg. Hold 30 seconds, then bend the back knee slightly to shift the stretch into the soleus. Repeat on both sides.
Sets/Reps: 3 × 30-second holds per position, per side
Common Mistakes: Allowing the heel to lift; rushing through the hold; stretching only the gastrocnemius and skipping the bent-knee soleus position.
Purpose: Forces the entire arch-support system — intrinsic muscles, posterior tibialis, ankle stabilizers — to work together under real bodyweight load.
How To Perform:
Stand on one foot. Maintain a soft knee, neutral foot alignment, and a level pelvis. Hold for 30 to 60 seconds. Progress by closing your eyes (increases proprioceptive demand) or standing on a folded towel or balance disc.
Sets/Reps: 3 × 30–60 seconds per side
Common Mistakes: Locking the standing knee; allowing the arch to fully collapse during the hold; using arms for excessive balance compensation. Watch that the ankle doesn't drift inward — this is the arch collapsing, and correcting it in real time is exactly the training effect you're after.
The evidence-based answer is: it depends on your symptoms, your arch type, and what you're trying to accomplish.
For symptomatic flexible flat feet, arch support — whether from footwear or from orthotics — consistently reduces pain and fatigue during standing and activity. A 2016 systematic review published in the British Journal of Sports Medicine found that foot orthoses significantly reduced pain in adults with flatfoot-related symptoms. The mechanism is straightforward: arch support shares the mechanical load that the foot's own structures are struggling to carry, reducing cumulative strain on the plantar fascia, posterior tibialis tendon, and surrounding tissues.
For asymptomatic flat feet — no pain, no fatigue, no functional limitation — there is no strong evidence that arch support is necessary or beneficial. The foot is managing its load without help.
Over-the-counter inserts vs. custom orthotics:
OTC options like Superfeet, Powerstep, or Currex work well for the majority of people with flexible flat feet. They're significantly less expensive than custom orthotics and, for most presentations, produce comparable outcomes.
Custom orthotics are most appropriate when biomechanical issues are complex, significant overpronation is involved, or several OTC options have failed to provide relief.
One important caveat: arch supports reduce load on the arch, but they do not strengthen the muscles that support it. Relying exclusively on orthotics without addressing intrinsic foot strength is a compensatory strategy, not a corrective one. The best approach combines appropriate support with the strengthening exercises above.
→ See Best Shoes for Flat Feet for footwear recommendations built around this principle.
Barefoot and minimalist footwear have earned real attention in foot health conversations, and the research around foot muscle activation in minimal shoes is genuinely interesting. Studies, including work by Goldmann and Brüggemann published in the Journal of Applied Biomechanics, have shown that walking in minimal footwear increases intrinsic foot muscle activity compared to conventional supportive shoes — potentially making the foot stronger over time.
For people with flat feet, this creates a tension worth thinking through carefully. The very thing that makes minimal shoes compelling — reduced external support — is also what makes them risky for arches that are already struggling to support themselves.
The answer isn't a blanket recommendation in either direction. It depends on where you are in the process.
Not everyone with flat feet is in the same situation. For some, minimalist shoes are a reasonable long-term goal. Specifically, people who fit this profile tend to respond well:
Mild, flexible flat feet with no active pain. If your arch is low but not fully collapsed, you have no current symptoms, and your flat feet are flexible (the arch returns when you sit), your foot musculature may be capable of handling the increased demand that minimalist shoes create. These are the ideal candidates for a gradual transition.
People who want to build foot strength proactively. Minimalist shoes are most valuable as a strengthening tool, not a treatment tool. If you're pain-free and want to build a more resilient arch over time, a slow, deliberate transition to lower-drop, wider-toe-box footwear can support that goal — provided it's paired with the intrinsic muscle exercises in Section 8.
Those already doing targeted foot strengthening. The research suggests that the benefit of minimal shoes compounds when intrinsic foot muscle training is already in place. Think of it this way: the shoes reduce the artificial support, and the muscles step in to fill the gap. That only works if the muscles have been built first.
For others, minimalist footwear in the near term is more likely to aggravate the problem than resolve it:
Active plantar fasciitis. The plantar fascia is already under elevated strain in flat feet. A minimalist shoe removes the arch support that was sharing that load. The result, especially on hard surfaces, can be a significant spike in plantar fascia tension and pain. This is one of the more common mistakes people make: switching to barefoot-style shoes thinking they'll strengthen their way out of plantar fasciitis, only to worsen it. → See What Is Plantar Fasciitis?
Posterior tibial tendon dysfunction. PTTD is the most common cause of adult-acquired flatfoot, and the posterior tibialis is already under strain. Minimalist footwear removes the external support that offloads this tendon. In the presence of active PTTD, this is contraindicated without professional guidance.
Severe or rigid flat feet. When the arch is significantly collapsed and does not return under unloaded conditions, the structural deficit is beyond what muscle activation alone can compensate for. Minimal footwear in this context places load on structures that have limited capacity to handle it.
Anyone transitioning too quickly. Even good candidates for minimalist shoes can injure themselves by moving too fast. The tendons, ligaments, and muscles of the foot adapt slowly. Transitioning from conventional supportive footwear to zero-drop minimalist shoes over a few weeks is a reliable way to develop Achilles pain, shin splints, or forefoot stress injuries — regardless of arch type.
If you've read the above and you fit the "might benefit" profile, here's the measured approach:
Start by simply wearing a lower-drop shoe rather than going fully zero-drop immediately. A 4–6mm drop shoe is a reasonable intermediate step from a conventional 10–12mm drop shoe. Wear it for daily activities — not extended walking sessions — for 4 to 6 weeks while continuing your intrinsic foot muscle exercises.
From there, gradually increase time in the lower-drop shoes while monitoring for any new symptoms. Achilles tightness after wearing them is a normal adaptation signal. Sharp new pain is not — back off if that appears.
True minimalist or zero-drop shoes should be the final destination, not the starting point. Give the process at least three to six months from your current footwear baseline.
The bottom line on barefoot shoes and flat feet: They're a tool, not a cure. Used correctly, they can build a stronger, more self-sufficient arch over time. Used prematurely or without proper conditioning, they add load to structures that are already under strain. Build the strength first. Then reduce the support.
→ See Barefoot Shoes Beginner Guide | Zero Drop Shoes Explained
Choosing the right shoe for flat feet isn't about finding the most cushioned option or the one with the most aggressive arch support. It's about matching the shoe's structural features to your specific presentation — the severity of your arch collapse, whether you're symptomatic, and what activities you're asking the shoe to support.
Here are the six variables that matter most.
For flat feet, arch support does something specific: it takes over part of the job that the plantar fascia, posterior tibialis, and intrinsic foot muscles are struggling to do on their own. A well-contoured arch support distributes load across the full plantar surface rather than concentrating it at the heel attachment and fascia origin.
What to look for: a firm, contoured footbed that makes contact with your arch when you're standing. A flat insole that doesn't rise to meet the arch isn't providing meaningful support regardless of what the marketing says.
This is one of the most underappreciated variables in flatfoot footwear. A narrow toe box compresses the forefoot, restricts the natural splay of the toes, and crowds the big toe inward — which, as covered in Section 6, increases the risk of bunion development over time in people with flat feet.
A wide toe box allows the toes to spread naturally with each step, which improves forefoot load distribution and reduces the inward force on the first metatarsophalangeal joint. For flat feet specifically, this is worth prioritizing even in supportive footwear.
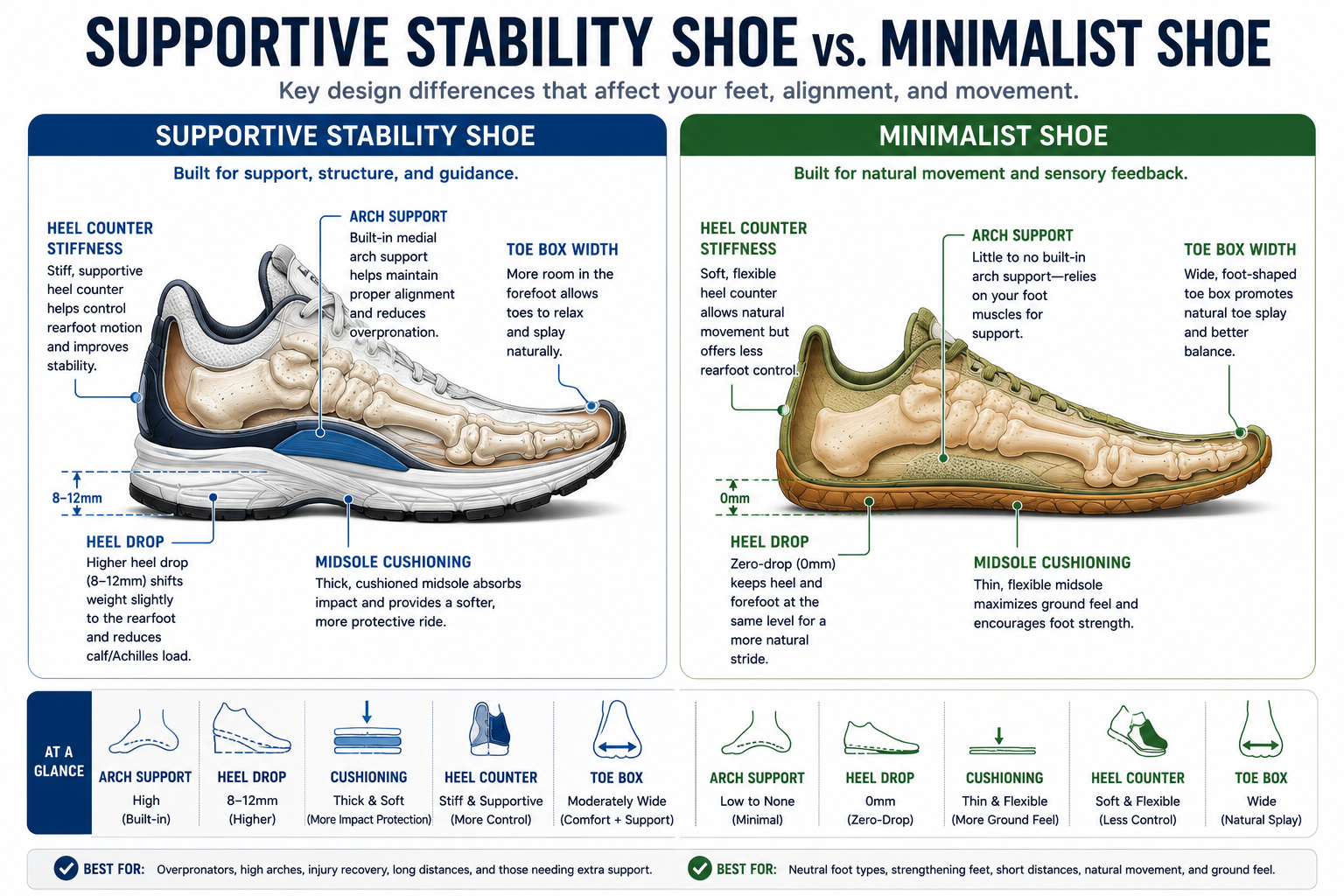
Overpronation — the inward rolling of the foot during walking — is common in flat feet. Stability shoes are designed to address this with a denser foam or TPU guide rail along the medial (inner) midsole that resists excessive pronation without completely blocking natural foot movement.
Motion control shoes take this further, with a stiffer last and firmer medial post. These are appropriate for severe overpronation but can feel rigid and may not be necessary for mild-to-moderate flat feet.
Adequate midsole cushioning reduces the ground reaction force that travels through the foot with each step. This is particularly relevant for flat feet because the arch — which normally absorbs and returns elastic energy — is less efficient in its role. The midsole has to compensate for some of that load.
Look for a midsole that compresses meaningfully when you press a thumb into it but rebounds rather than staying compressed. A midsole that doesn't spring back has likely been compacted and is no longer performing its function.
Heel drop is the height difference between the heel and the forefoot. Most conventional supportive shoes sit at 8–12mm of drop. Zero-drop shoes sit level.
For flat feet, a moderate heel drop (6–10mm) can help by reducing the demand on the calf-Achilles complex and, by extension, reducing tension on the plantar fascia. Very high heel drop can shorten the calf over time, which creates a secondary problem. Very low or zero drop places greater demand on intrinsic foot structures — appropriate once strength is built, premature before it is.
Supportive stability shoes are almost always the right starting point for symptomatic flat feet. They offload strained structures, reduce pain, and allow active recovery through exercise. Minimalist or barefoot-style shoes are a long-term option for people who want to build foot strength progressively — not a first-line intervention.
The two approaches aren't mutually exclusive. Many people with flat feet wear supportive footwear for work and daily activity while incorporating shorter periods in minimal shoes as a strengthening stimulus, under the guidance of a clinician or once they've built a solid foundation through intrinsic muscle training.
→ Read our complete guide to the Best Shoes for Flat Feet for specific brand and model recommendations vetted for this condition.
Flat feet are manageable with self-directed care in most cases. But certain signs indicate that professional evaluation should come before home treatment.
See a podiatrist, orthopedic specialist, or physical therapist if:
A clinical evaluation for flat feet typically includes assessment of arch height and flexibility, range of motion testing, posterior tibial tendon function, gait observation, and potentially imaging to rule out bony abnormalities.
Are flat feet genetic?
Yes, in many cases. The arch development process is influenced by genetics, including the inherent laxity of your ligaments, the shape of your tarsal bones, and the length of your Achilles tendon. If one or both of your parents have flat feet, your likelihood of developing them is higher. That said, genetics set a predisposition, not a destiny. Muscle strength and footwear choices have meaningful influence over whether flat feet become symptomatic.
Can flat feet cause plantar fasciitis?
Yes. Flat feet are one of the established risk factors for plantar fasciitis because arch collapse places repetitive tensile stress on the plantar fascia with every step. Not everyone with flat feet develops plantar fasciitis, but the mechanical relationship is well-documented. → See What Is Plantar Fasciitis?
Do flat feet get worse with age?
They can. The structures that support the arch — ligaments, tendons, intrinsic muscles — are subject to cumulative loading over decades. Without strength training and appropriate footwear, progressive flattening is common, particularly in the 40s and 50s. Posterior tibial tendon dysfunction, one of the most common causes of adult-acquired flatfoot, becomes more prevalent with age.
Can adults rebuild their arches?
Partially, in many cases. Research demonstrates that targeted intrinsic foot muscle training can increase navicular height (a measure of arch height) in adults with flexible flat feet. The arch will not become structurally normal through exercise, but functional improvements are real, measurable, and clinically meaningful. Pain and fatigue can improve significantly even when arch height changes modestly.
Are barefoot shoes good for flat feet?
Potentially, but not immediately. Barefoot shoes can help build the foot strength that supports the arch over time. However, people with flat feet are at greater risk of overloading the plantar fascia and posterior tibialis during the transition period. Start with supported footwear, build intrinsic foot strength for several months, then reduce support gradually. → See Barefoot Shoes Beginner Guide
Do I need orthotics if I have flat feet?
Not necessarily. Asymptomatic flat feet — those not causing pain or functional limitation — do not require orthotics. For symptomatic flat feet, orthotics are a valuable tool for reducing pain and fatigue, but they work best as part of a strategy that also includes strengthening. Orthotics support the arch; exercise builds the structures that hold it up from within.
Most people with flat feet spend years treating their knees, their back, or their general foot fatigue — without ever connecting the dots back to what's happening at the arch. That's the part worth getting right.
Flat feet are common, varied in their presentation, and far more treatable than most people assume. Whether you have flexible arches that fatigue by midday or a more significant collapse that's been reshaping your gait for years, the intervention options are real and evidence-backed.
Start with the fundamentals. Build intrinsic foot strength through short foot exercises and single-leg balance work. Pair that with appropriate footwear that shares the mechanical load your arch is struggling with. And if arch supports are part of your current strategy, let them be a bridge to greater foot strength, not a permanent substitute for it.
The arch has muscles behind it. Train them, and the arch tends to take care of itself.
Continue Reading:
→ What Is Plantar Fasciitis?→ Overpronation Explained→ Foot Pain Location Guide→ Best Shoes for Flat Feet→ Barefoot Shoes Beginner Guide→ Foot Strengthening Exercises for Plantar Fasciitis
Medical Disclaimer: This content is for educational purposes only and does not constitute medical advice. If you are experiencing persistent or worsening foot pain, consult a qualified healthcare provider.
Research References:
Makris EA et al. "Prevalence of flatfoot in adults." Journal of the American Podiatric Medical Association, 2016.
Tenenbaum S et al. "Flexible flatfoot in adults: an overview." Foot & Ankle Specialist, 2013.
Headlee DL et al. "Fatigue of the plantar intrinsic foot muscles increases navicular drop." Journal of Electromyography and Kinesiology, 2008.
Lynn SK et al. "Minimalist running shoes and intrinsic foot muscle activation." Journal of Applied Biomechanics, 2012.
Mickle KJ et al. "Relationship between body mass index and flatfoot in adults." Journal of the American Podiatric Medical Association, 2006.
Kulig K et al. "Selective activation of tibialis posterior: elevation and eccentricity." Journal of Orthopaedic and Sports Physical Therapy, 2004.
Rao UB, Joseph B. "The influence of footwear on the prevalence of flat foot." Journal of Bone and Joint Surgery (British), 1992.
Cheung RT et al. "Foot orthoses and their effect on flatfoot symptoms." British Journal of Sports Medicine, 2016.