Learn what bunions are, what causes them, how they progress, and the most effective treatment options. Discover the connection between foot structure, footwear, flat feet, and bunion development.
If you've noticed a bump forming at the base of your big toe, and it's started pushing your big toe toward your other toes, you're probably dealing with a bunion. It's one of the most common foot conditions out there, and yet most people don't really understand what's happening inside their foot until the pain shows up and the shoe shopping gets harder.
The medical term for a bunion is hallux valgus. "Hallux" is just the medical word for your big toe, and "valgus" describes the outward angle it drifts toward. Once you know that, the rest of the terminology starts to make a lot more sense.
Here's the part most articles skip: a bunion isn't just a bump. It's a structural shift in the bones of your foot, and once it starts, it tends to get worse without some kind of intervention. That doesn't mean surgery is inevitable. It means the earlier you understand what's driving it, the more control you have over how it progresses.
This guide walks through what's actually happening at the joint, why bunions form, how to tell which stage yours is at, what treatments genuinely help, and when surgery becomes the right call instead of a last resort. By the end, you'll know more about bunions than most people learn from a five-minute doctor's visit.
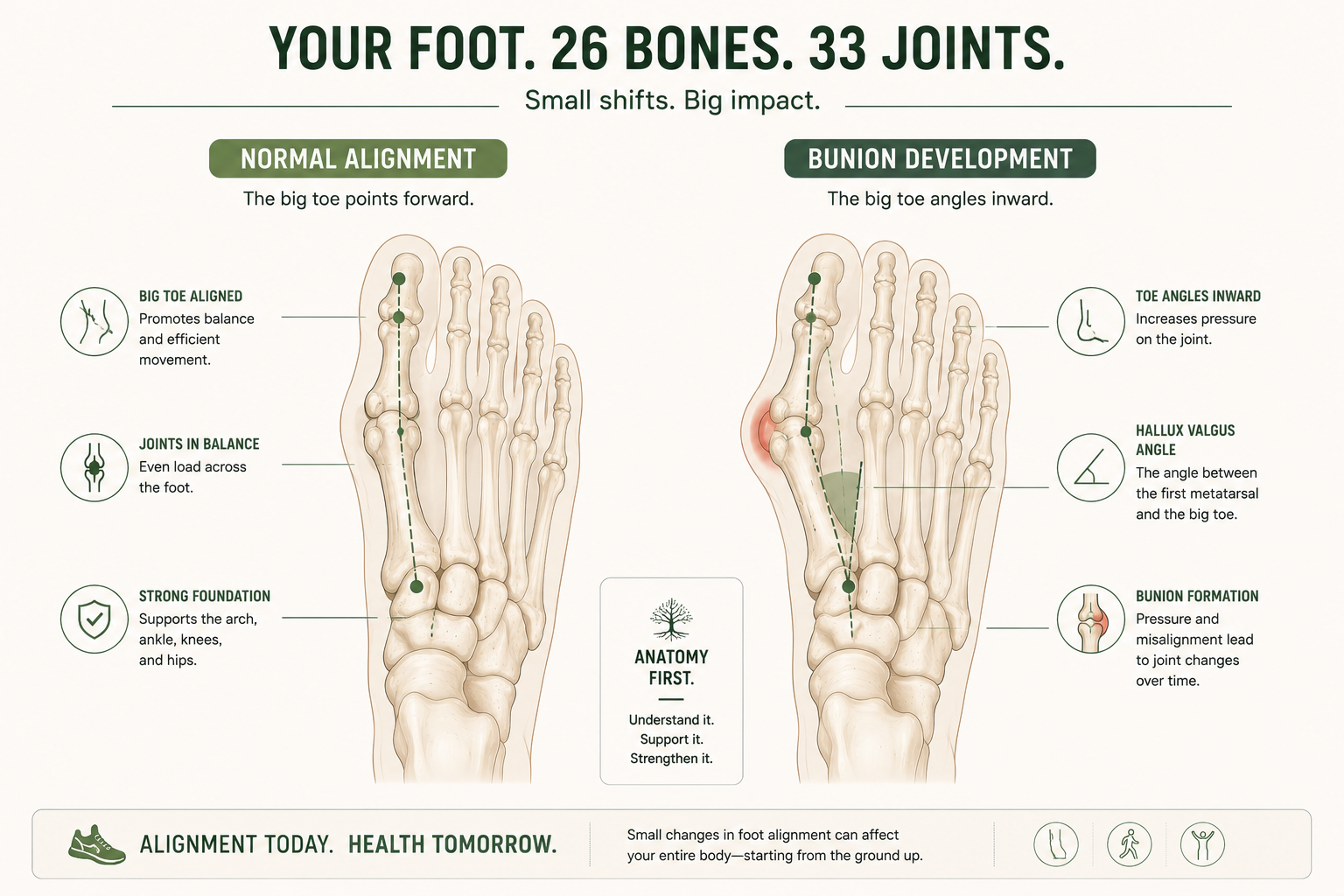
A bunion is a bony bump at the base of the big toe, caused by a structural shift in the joint where the big toe meets the foot. The toe angles inward while the joint pushes outward, and doctors call this hallux valgus. Bunions are progressive, meaning they tend to worsen over time, and they can't be reversed without surgery. Genetics and foot structure are the main causes, with tight or narrow footwear speeding up progression rather than starting it. Wide toe box shoes, foot-strengthening exercises, and toe spacers can ease pain and slow things down. Surgery is reserved for bunions causing real pain or functional limits, not just for how they look.
Bunions are far more common than most people realize. A 2010 systematic review and meta-analysis by Nix, Smith, and Vicenzino, published in the Journal of Foot and Ankle Research, pooled data across dozens of population studies and found that hallux valgus affects approximately 23% of adults between 18 and 65, climbing to roughly 36% of adults over 65. The same review found bunions affect close to 30% of adult women, making them noticeably more common in women than men across nearly every age group studied.
Why prevalence increases with age. Bunions are progressive by nature, so the longer a person lives with the underlying structural tendency, the more time the deformity has to advance. Years of cumulative joint stress, naturally loosening ligaments, and decades of footwear choices all stack on top of each other, which is why the jump from middle age to the senior years is so pronounced in the data.
Why women are affected more often. Researchers point to a few overlapping factors: differences in female foot shape and ligament laxity, hormonal influences on connective tissue, and historically higher rates of narrow or heeled footwear use. A heritability study by Hannan and colleagues, published in Arthritis Care & Research in 2013 using data from the Framingham Foot Study, found hallux valgus to be highly heritable in both men and women, with heritability estimates around 0.29 overall and rising to 0.45 in adults between 39 and 60. In plain terms, genetics explain a substantial share of who develops a bunion, but they don't explain the whole picture, which is where sex differences in footwear history and connective tissue come in.
The bottom line. If you have a bunion, you're in very good company. This isn't a rare or unusual diagnosis. It's one of the most prevalent structural foot conditions in adult populations worldwide, and the data shows it only becomes more common as we age.
A bunion is a structural deformity of the big toe joint, where the first metatarsal drifts outward and the big toe angles inward, creating a visible bump on the inside edge of the foot. It develops gradually as the bones, ligaments, and tendons around the joint shift out of their normal position.
Your big toe joint, formally called the first metatarsophalangeal joint (or MTP joint for short), is where your big toe bone meets the long bone that runs back into your midfoot. In a healthy foot, that joint sits in a straight line. The big toe points forward, and the metatarsal bone behind it stays aligned with the rest of your foot.
To really understand what's shifting, it helps to know the individual parts involved. The first metatarsal is the long bone that runs from the middle of your foot out to the base of your big toe. It's the foundation the whole joint is built on. The proximal phalanx is the first bone of the big toe itself, the one that connects directly to the metatarsal and does most of the bending when you walk or push off the ground. Where these two bones meet is the first metatarsophalangeal joint, the hinge that lets your big toe flex with every step.
Surrounding that joint is the joint capsule, a fibrous sleeve that holds the joint together and keeps the bones properly seated against each other. Wrapping around the outside of the capsule are ligaments, tough bands of connective tissue that resist excessive movement and keep the joint stable side to side. Running through and around the joint are tendons, the cord-like structures that connect muscle to bone and actually generate the pulling force that moves the toe.
In a bunion, this entire system gets pulled out of balance. As the first metatarsal drifts outward and the proximal phalanx angles inward, the joint capsule stretches on one side and tightens on the other. The ligaments that used to hold everything centered start pulling at an angle instead of straight, which actually reinforces the deformity over time rather than correcting it. The tendons that flex and extend the big toe shift their line of pull too, so the same muscles that used to move the toe straight forward now contribute to dragging it further out of alignment with every step.
A bunion happens when that alignment breaks down. The metatarsal bone drifts outward, away from the other toes, while the big toe itself tilts inward, toward the second toe. The joint where these two bones meet gets pushed out to the side, and that's the bump you're seeing and feeling. It's not a growth or extra bone tissue. It's your existing joint, shifted into a new position.
Think of it like a tent pole that's slowly leaning. The pole itself isn't broken, but as the angle shifts, the fabric around it bunches and strains in ways it wasn't designed to. Your big toe joint works the same way. As the bones angle apart, the soft tissue, the joint capsule, and eventually the joint surface itself all start to feel the strain.
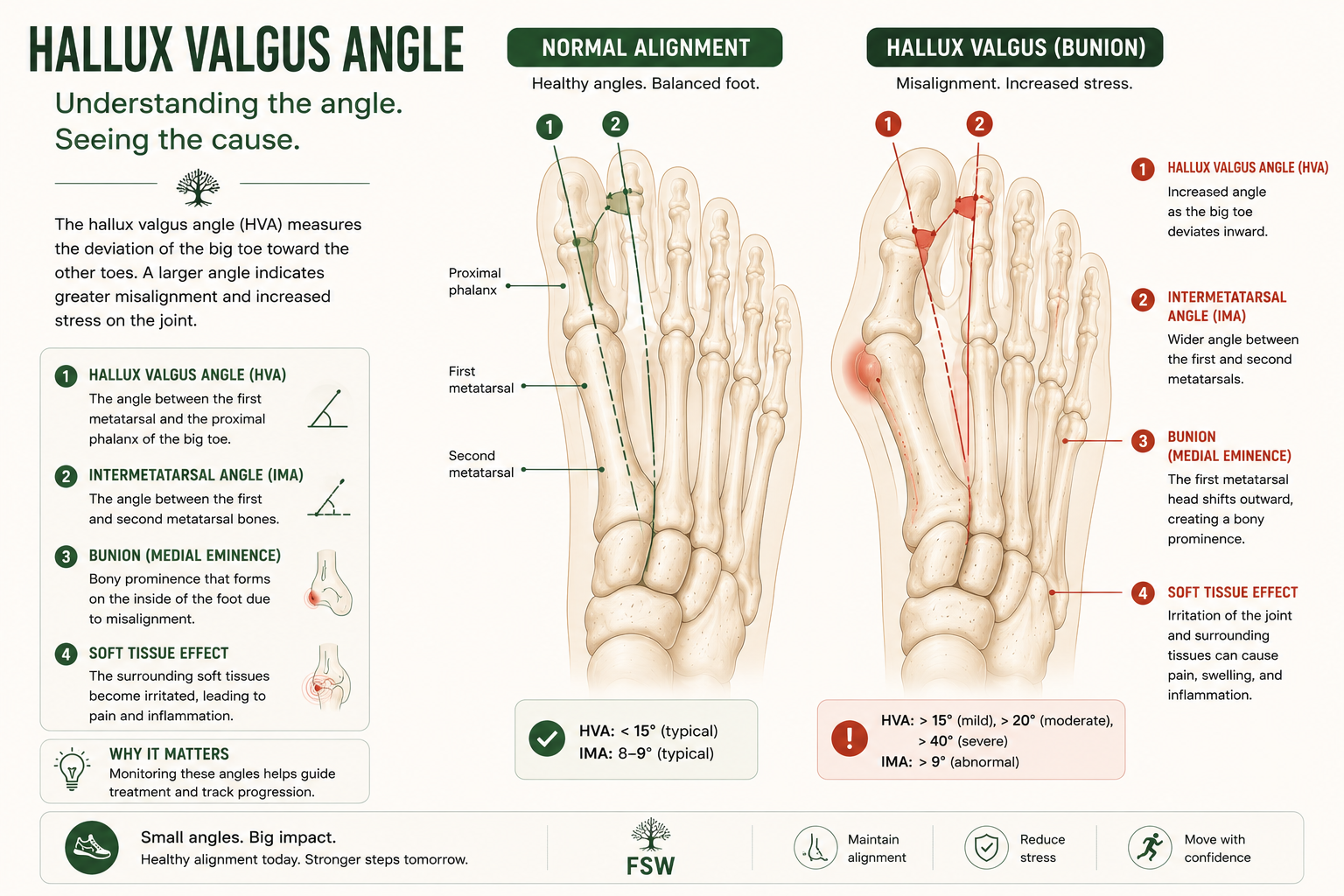
Doctors actually measure this shift with a specific number called the hallux valgus angle, which is the angle formed between the first metatarsal and the proximal phalanx on an X-ray. A healthy angle sits under about 15 degrees. As that number climbs into the high teens, twenties, and beyond, the bunion moves from mild to moderate to severe, and the mechanical disadvantage on the joint compounds. Once the angle gets large enough, the tendons and ligaments are pulling from such an altered position that the deformity tends to feed on itself, which is part of why bunions rarely improve without some kind of intervention.
This is why the medical community uses the term hallux valgus rather than just calling it "bunion bump." Hallux valgus describes the deviation, the actual mechanical shift. The bump is just the visible result of that shift.
Bunions are caused mainly by inherited foot structure and genetics, which determine how stable the big toe joint is to begin with. Flat feet, joint hypermobility, and arthritis can speed up the process, and tight or narrow footwear accelerates progression in feet that are already predisposed, though it isn't a root cause on its own.
Bunions rarely come from a single cause. They're usually the result of several factors working together over years, sometimes decades, before the bump becomes noticeable.
Foot structure is inherited, and that includes the traits that make someone more prone to bunions. The Framingham Foot Study, led by Hannan and colleagues and published in Arthritis Care & Research in 2013, examined thousands of adults and found hallux valgus to be highly heritable, with genetics accounting for roughly 29% to 45% of the variation in who develops the condition depending on age group. If your mother or grandmother had bunions, your odds of developing them go up substantially, independent of what shoes you wear.
This is also why bunions tend to run in families even when lifestyle and footwear habits are completely different between generations. One thing that surprises a lot of patients: a parent or grandparent's bunion often looked nothing like theirs at the same age, because the rate and pattern of progression varies even within the same family line.
Some people are simply built with a foot shape that puts more stress on the big toe joint. A longer first metatarsal, looser ligaments around the joint, or an unusual gait pattern can all shift more force onto that joint with every step you take. Over tens of thousands of steps a year, even small structural differences compound into visible changes.
Flat feet and bunions are mechanically connected, mainly through a pattern called overpronation that increases stress on the big toe joint. We'll cover exactly how that connection works in the next section, since it's significant enough to deserve its own explanation.
This is where a lot of people get the cause-and-effect backwards. Shoes do not directly cause bunions. You can't develop hallux valgus purely from wearing the wrong shoe if your foot structure wasn't already predisposed to it.
What footwear does do is accelerate the timeline. Narrow toe boxes and high heels push the toes into the same inward position that a bunion creates naturally, which speeds up the joint's drift and increases pain along the way. Twin studies on hallux valgus consistently find that shared genetics explain most of the variance in who develops bunions, with lifetime footwear habits acting as an accelerant rather than a root cause.
So the honest answer is: footwear is a contributing factor, not the root cause. Someone with no genetic or structural predisposition can wear narrow shoes their whole life and never develop a bunion. Someone with a strong predisposition will likely develop one regardless of footwear, but bad shoes will get them there faster and make it hurt more along the way. A common misconception is that going barefoot or wearing flip-flops constantly will prevent a bunion. It won't, if the underlying predisposition is there, though it also won't accelerate things the way a narrow pump would.
Inflammatory types of arthritis, particularly rheumatoid arthritis, can damage the joint capsule and surrounding ligaments in ways that destabilize the big toe joint. This type of bunion tends to progress faster and is often accompanied by more significant joint damage than bunions caused by structural or genetic factors alone.
Some people have naturally loose, hypermobile joints throughout their body, not just in their feet. This connective tissue laxity means the ligaments holding the big toe joint in place don't resist the outward drift as effectively, allowing the deformity to progress more easily and often at a younger age than typical bunion cases.
Flat feet deserve their own closer look here, because the mechanical chain connecting them to bunions is one of the most underexplained relationships in foot health content.
Arch collapse. A healthy arch acts like a spring, absorbing impact and distributing weight evenly as you move through each step. When the arch flattens, that spring mechanism breaks down, and the foot has to find other ways to manage the same forces.
Overpronation. Without a functioning arch, the foot tends to roll inward excessively during the stance phase of walking, a pattern called overpronation. This rolling motion shifts how your body weight travels through the foot on its way out through the toes.
First ray instability. The "first ray" refers to the first metatarsal and big toe working as a single functional unit. In a flat, overpronated foot, this unit becomes less stable, allowing the first metatarsal more freedom to drift out of alignment than it would in a foot with a stable arch holding everything in place.
Increased pressure through the first MTP joint. All of this adds up to one outcome: more repetitive stress concentrated directly on the first metatarsophalangeal joint with every step. Over years, that excess pressure becomes one of the more significant mechanical contributors to bunion development and progression.
One clinical pearl worth knowing here: a lot of people treat their flat feet and their bunion as two separate problems when they show up together. In reality, addressing the arch collapse is often the single highest-leverage move available, because it reduces the mechanical driver feeding the bunion rather than just managing the bunion's symptoms in isolation.
If this pattern sounds familiar, our full guide on what are flat feet goes deeper into the biomechanics, including how arch collapse develops in the first place and what actually helps.

Not every bunion is the same kind of bunion. While the traditional bump at the base of the big toe is the most familiar, there are a few distinct variations worth knowing about, especially if your bump doesn't quite match the typical description.
This is the classic bunion described throughout this guide: a structural shift at the first metatarsophalangeal joint where the big toe angles toward the second toe and the metatarsal pushes outward. It develops gradually, usually over years, and is driven primarily by genetics and foot structure.
Juvenile bunions follow the same basic mechanics as the traditional adult version, but they show up much earlier, sometimes as young as 10 to 15 years old. They tend to run strongly in families and are often associated with flexible flat feet and loose ligaments during growth years. Because there's more growth and development ahead, treatment approaches in younger patients lean more conservative for longer before surgery is considered.
A tailor's bunion forms at the opposite end of the foot, at the base of the little toe instead of the big toe. The fifth metatarsal bone drifts outward in a similar way to how the first metatarsal drifts in a traditional bunion, creating a bony bump on the outside edge of the foot. It gets its name from old tailors who sat cross-legged for long hours, putting repetitive pressure on the outside of their feet.
TypeLocationWho It Commonly AffectsTypical CauseTreatment ConsiderationsTraditional Bunion (Hallux Valgus)Base of big toe, inside edge of footAdults, more common in women and with ageGenetics, foot structure, footwear as accelerantWide toe box shoes, orthotics, exercises, surgery if severeJuvenile BunionBase of big toe, inside edge of footChildren and adolescents, often with family historyStrong heredity, flexible flat feetConservative management preferred during growth yearsTailor's Bunion (Bunionette)Base of little toe, outside edge of footAdults, often with a genetically narrow forefootFifth metatarsal misalignment, footwear pressureWide shoes, padding, surgery in persistent cases

Bunion symptoms vary quite a bit depending on how far the joint has shifted. Here's what most people notice, in roughly the order they tend to show up.
Visible bump
A firm, bony protrusion at the base of the big toe, on the inside edge of the foot.
Pain
Aching or sharp pain at the joint, often worse in tight shoes or after standing.
Swelling
Puffiness and inflammation around the joint, sometimes warm to the touch.
Redness
Skin irritation directly over the bump from shoe friction.
Restricted motion
Stiffness when trying to bend the big toe up or down.
Calluses
Thickened skin where the bunion or shifted toes rub against shoes or each other.
Difficulty fitting into shoes
Shoes that used to fit now feel tight specifically across the widest part of the foot.
Not everyone experiences pain early on. Some people walk around with a visible bunion for years before it ever actually hurts. Pain tends to show up once the joint surfaces start rubbing against each other differently, or once the bump itself becomes large enough to create constant friction inside regular shoes. Many people don't realize the bump and the pain are somewhat independent variables. A large, visually obvious bunion can be nearly painless, while a smaller one might ache constantly.
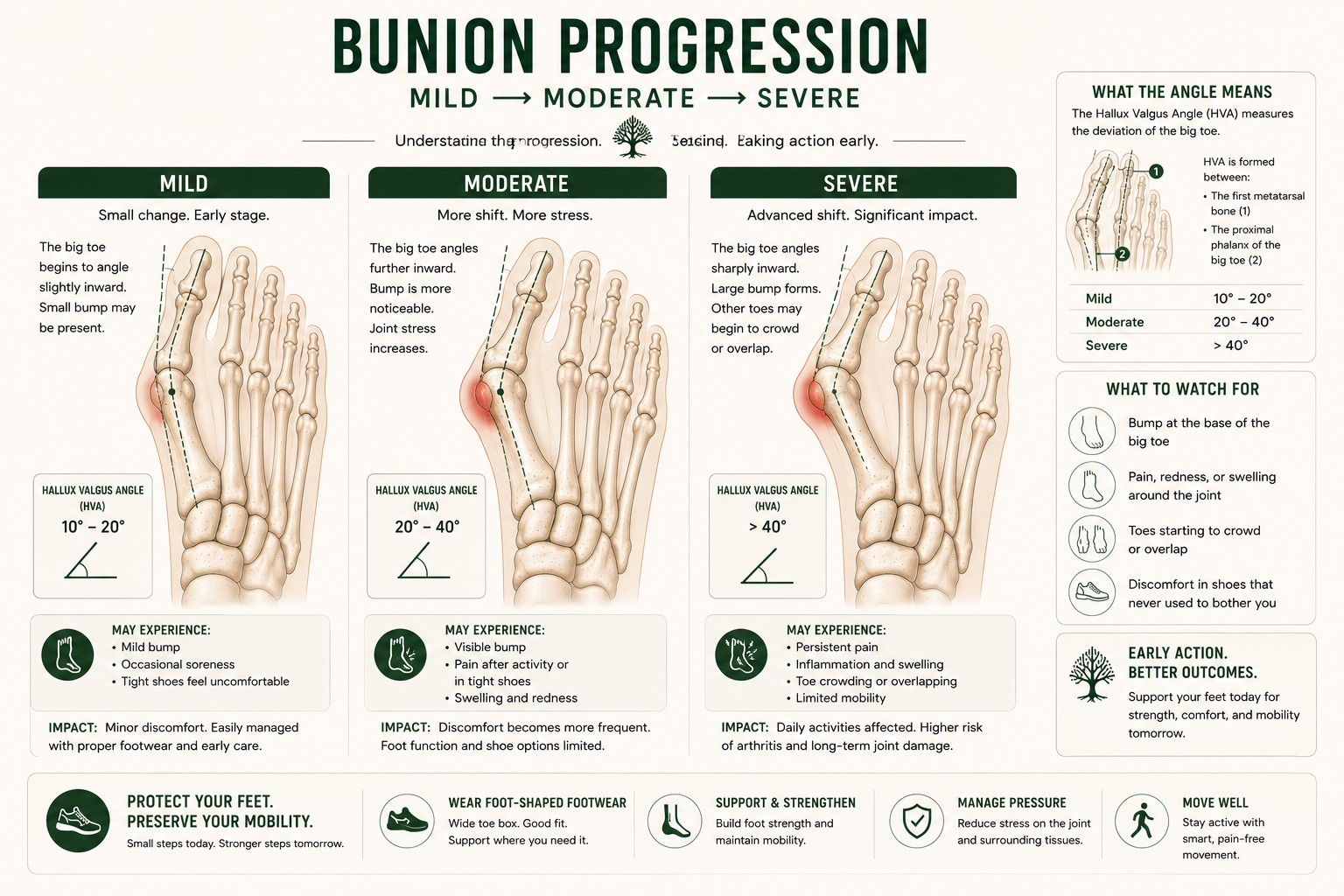
Bunions are typically described in three stages, based on how far the big toe has angled and how much the joint structure has changed.
Mild
Toe Position: Slight inward angle, bump barely visible
Symptoms: Little to no pain, occasional shoe tightness
Daily Impact: Minimal; most regular shoes still fit
Moderate
Toe Position: Noticeable inward angle, visible bump
Symptoms: Intermittent pain, redness, and mild swelling
Daily Impact: Shoe shopping becomes more difficult, and certain activities may cause discomfort
Severe
Toe Position: Significant inward deviation, sometimes overlapping the second toe
Symptoms: Persistent pain, joint stiffness, and callus formation
Daily Impact: Walking and standing can become difficult, with very limited footwear options available
The rate of progression varies enormously from person to person. Some bunions stay mild for decades. Others move from mild to moderate within just a few years, especially if the underlying cause (like uncontrolled flat feet or a fast-progressing hereditary pattern) isn't addressed at all.
The stages described above (mild, moderate, severe) are useful shorthand, but doctors actually rely on two specific angle measurements to quantify exactly how far a bunion has progressed.
Hallux Valgus Angle (HVA). This is the angle formed between the long axis of the first metatarsal and the long axis of the proximal phalanx, measured on a weight-bearing X-ray. It's the primary number used to track how far the big toe itself has drifted.
Intermetatarsal Angle (IMA). This measures the angle between the first and second metatarsal bones. Where the HVA tells you how far the toe has angled, the IMA tells you how far the underlying metatarsal has spread away from its neighbor, which is a separate but related part of the deformity.
SeverityHallux Valgus AngleNormalUnder 15 degreesMild15 to 20 degreesModerate20 to 40 degreesSevereOver 40 degrees
Why angles matter. These measurements give doctors an objective, reproducible way to track a bunion over time and compare it against population data, rather than relying purely on visual impression. They also directly inform which surgical approach makes sense if surgery becomes necessary, since different procedures are built to correct different degrees of angular deformity.
How doctors use them. At a typical evaluation, a podiatrist or orthopedic surgeon will use these angles together with the physical exam to build a complete picture. A patient with a high HVA but a relatively low IMA might be a candidate for a different procedure than someone whose IMA is significantly elevated, because the angles point to slightly different mechanical problems within the joint.
Why symptoms matter more than numbers alone. Here's the clinical pearl most patients never hear: angle severity and symptom severity don't always move together. It's entirely possible to have a moderate HVA with minimal pain, or a mild HVA with significant discomfort, depending on individual anatomy, activity level, and footwear. Treatment decisions, especially around surgery, should be driven primarily by how the bunion is actually affecting your life, not by chasing a specific number on an X-ray.
Diagnosing a bunion is usually straightforward and doesn't require advanced imaging in most cases.
Physical examination. A doctor or podiatrist will look at the alignment of your toe, check the range of motion in the joint, and press around the area to assess pain, swelling, and skin condition. They'll also watch how you walk, since gait often reveals how the bunion is affecting your overall mechanics.
X-rays. Imaging becomes useful when a doctor needs to measure the exact angle of deviation, which helps determine the severity stage and guides treatment decisions, especially if surgery is being considered. X-rays also rule out other joint issues, like arthritis changes, that might be contributing to the symptoms.
When imaging is necessary. If your bunion is mild and not particularly painful, you likely won't need an X-ray. If you're experiencing significant pain, considering surgical options, or your doctor suspects arthritis is involved, imaging becomes a standard next step.
No, bunions cannot be reversed without surgery. Once the bones of the big toe joint shift into a hallux valgus position, no exercise, stretching, or device can move them back permanently. Conservative treatments like wide shoes, toe spacers, and strengthening exercises can reduce pain and slow progression, but only surgery physically corrects the joint's alignment.
Once the bones of the big toe joint have shifted into a hallux valgus position, no amount of stretching, exercise, or non-surgical treatment will physically move them back into their original alignment. The only way to structurally correct the bone position is surgery.
A lot of people find this hard to believe, especially with so much marketing around toe spacers, splints, and "bunion correctors" that imply otherwise. Here's the more accurate picture.
Why structural changes can't be reversed naturally. The bones, ligaments, and joint capsule have already adapted to the new position. Soft tissue stretching or splinting can temporarily reposition the toe while it's being worn, but as soon as it's removed, the underlying bone structure pulls it right back. There's no non-surgical method that creates a permanent change in bone alignment.
What conservative treatment can actually improve. Pain, inflammation, and the rate of progression. Wide toe box shoes reduce friction and pressure. Strengthening exercises can improve the stability of the muscles supporting the joint. Toe spacers can offer temporary relief and may slow the rate of progression in early-stage bunions, though they won't undo existing deformity.
Realistic expectations. If your bunion is mild, the right combination of footwear and exercise can keep it from progressing quickly and may keep you comfortable indefinitely without ever needing surgery. If your bunion is already moderate to severe, conservative treatment is about managing pain and slowing progression, not reversing what's already happened.
Can bunions be corrected without surgery? No, not in the sense of restoring the joint to its original position. Non-surgical treatment can reduce pain, slow how quickly the deformity progresses, and improve comfort in daily life, but it cannot move the bones back into proper alignment. Surgery is the only method that physically corrects the structural position of the joint. For many people with mild to moderate bunions, that distinction doesn't matter much in practice, since conservative care is often enough to manage symptoms long term.
What it does: Reduces pressure and friction on the bunion by giving the forefoot room to sit naturally without being compressed.
What it does not do: Change the underlying bone alignment.
Level of scientific support: Strong. Multiple podiatric studies, including research published through the American Orthopaedic Foot & Ankle Society, consistently identify footwear modification as the first-line conservative intervention for symptomatic bunions.
What it does: Custom or over-the-counter orthotics can correct underlying biomechanical issues, like overpronation, that contribute to bunion progression, and they redistribute pressure away from the joint.
What it does not do: Reverse the existing bunion structure.
Level of scientific support: Moderate to strong, particularly when overpronation or flat feet are a contributing factor.
What it does: Creates temporary separation between the big toe and second toe, which can relieve pressure and improve comfort during wear.
What it does not do: Provide a permanent correction once removed.
Level of scientific support: Limited but promising for symptom relief; not supported as a structural treatment.
What it does: Improves joint mobility, reduces compensatory strain on surrounding muscles, and can address gait abnormalities contributing to the bunion's progression.
What it does not do: Eliminate the bunion itself.
Level of scientific support: Moderate, with growing evidence specifically for early-stage intervention.
What it does: Builds strength in the intrinsic foot muscles, which can improve joint stability and potentially slow progression in mild cases.
What it does not do: Correct existing structural deviation.
Level of scientific support: Emerging but encouraging. A 2026 randomized controlled trial by Meh, Pešič, and Kozinc, published in Applied Sciences, tested a six-week intrinsic foot muscle strengthening program in healthy adults and found it improved active hallux range of motion, ankle dorsiflexion, and modestly reduced hallux valgus angle. The study population didn't have diagnosed bunions, so the findings point to strengthening as a promising preventive and supportive measure rather than direct proof it treats an existing deformity. Adding a silicone toe spacer to the program didn't produce additional benefit over exercise alone.
What it does: Reduces repetitive stress on the joint from high-impact activities that may be accelerating irritation.
What it does not do: Address the root structural cause.
Level of scientific support: Practical and widely recommended, though more about symptom management than disease modification.
What it does: Over-the-counter NSAIDs and ice can reduce pain and swelling during flare-ups.
What it does not do: Slow or stop bunion progression.
Level of scientific support: Strong for short-term symptom relief; not a long-term solution.
These exercises won't undo a bunion, but they can meaningfully improve comfort, joint mobility, and the stability of the muscles around the joint. Consistency matters more than intensity here.
Purpose: Strengthens the muscles that spread the toes apart, helping counteract the inward pull on the big toe.
How To: Sit with your foot flat on the floor. Try to spread all five toes apart as wide as possible without curling them. Hold for 5 seconds, then relax.
Sets & Reps: 2 sets of 10 repetitions, once or twice daily.
Common Mistakes: Curling the toes instead of spreading them, or only moving the big toe while the others stay still.
Purpose: Activates the muscles that support the arch, which helps reduce the overpronation that often contributes to bunion progression.
How To: While seated with your foot flat, try to shorten your foot by drawing the ball of your foot toward your heel without curling your toes. You should feel the arch lift slightly.
Sets & Reps: 2 sets of 10, held for 5 seconds each.
Common Mistakes: Curling the toes to fake the movement instead of actually engaging the arch muscles.
Purpose: Builds strength in the small muscles along the bottom of the foot, supporting overall joint stability.
How To: Place a small towel on the floor in front of your foot. Using only your toes, scrunch the towel toward you.
Sets & Reps: 2 to 3 sets per foot, several times a week.
Common Mistakes: Using the whole foot to drag the towel rather than isolating toe movement.
Purpose: Maintains range of motion in the big toe joint, which tends to stiffen as a bunion progresses.
How To: Using your hand, gently pull your big toe into proper alignment and hold, then gently move it up and down through its natural range.
Sets & Reps: 10 repetitions, once or twice daily.
Common Mistakes: Forcing the stretch too aggressively, which can irritate an already sensitive joint.
Surgery becomes a reasonable option when a bunion is causing significant pain or functional limitation that hasn't responded to conservative treatment, not simply because a bump is visible.
When surgery becomes appropriate. Persistent pain that interferes with daily activities, difficulty finding any shoes that fit comfortably, or progressive joint damage are the main indicators. A bunion that's purely cosmetic, with no real pain or functional limitation, generally doesn't need surgical correction.
Common procedures. The general category is called a bunionectomy, but that term covers several distinct surgical approaches. The right one depends on how severe the deformity is, whether arthritis is present, and how stable the joint is overall.
An osteotomy is the most common bunion procedure. The surgeon cuts the first metatarsal bone and shifts it back into proper alignment, then secures it with small screws or pins while it heals. This is typically the go-to approach for mild to moderate bunions where the joint itself is still healthy.
The Lapidus procedure goes a step further by fusing the joint where the first metatarsal meets the midfoot, not just realigning the bone. It's generally reserved for more severe bunions or cases where there's excessive mobility at that joint contributing to the deformity, since fusing it provides a more stable, long-term correction.
An exostectomy is the simplest of the surgical options. The surgeon shaves down the bony bump itself without realigning the underlying joint. Because it addresses the visible symptom rather than the structural cause, it's used far less often today and typically only in very specific, mild cases, frequently alongside another procedure rather than on its own.
In cases involving significant arthritis or a severely damaged joint, surgeons may recommend fusing the big toe joint entirely, eliminating motion at that joint to eliminate the pain associated with it. This is a more significant procedure typically reserved for advanced cases where joint-preserving options aren't expected to hold up.
Osteotomy
Best For: Mild to moderate bunions with a healthy joint
Recovery Time: 6 to 8 weeks
Key Considerations: Most common bunion procedure; realigns the bone while preserving joint motion.
Lapidus Procedure
Best For: Moderate to severe bunions with midfoot instability
Recovery Time: 8 to 12 weeks non-weight-bearing, with 4 to 6 months for full activity
Key Considerations: Provides the most stable long-term correction but typically requires the longest recovery period.
Exostectomy
Best For: Very mild bunions, often performed alongside another procedure
Recovery Time: 4 to 6 weeks
Key Considerations: Removes the visible bump but does not correct the underlying bone alignment.
Fusion Procedures
Best For: Severe bunions with significant arthritis or joint damage
Recovery Time: Approximately 10 to 12 weeks
Key Considerations: Eliminates motion at the joint to relieve pain and is generally reserved for advanced cases.
Recovery expectations. Recovery typically takes anywhere from 6 to 12 weeks before returning to normal activity, with full recovery and swelling resolution sometimes taking up to a year. Most patients are in a protective boot or special shoe for several weeks post-surgery.
Success rates. According to data referenced by the American Academy of Orthopaedic Surgeons, the majority of bunion surgeries result in significant pain relief and improved function, though outcomes depend heavily on the severity of the original deformity and the specific procedure used.
Risks. As with any surgery, risks include infection, stiffness, nerve irritation, and in some cases, recurrence of the bunion over time, particularly if the underlying biomechanical cause (like uncorrected overpronation) isn't also addressed. Clinicians often see better long-term outcomes when patients address the mechanical root cause after surgery rather than assuming the procedure alone solved the underlying problem.
Surgery should be based on symptoms and function, not appearance alone. This is worth repeating because it's the single most important piece of guidance from foot and ankle surgeons. A bunion that doesn't hurt and doesn't limit your life is not a medical emergency, regardless of how it looks.
A bunion rarely stays contained to just the big toe joint. Left unaddressed, it tends to set off a chain reaction through the rest of the foot and, in some cases, up through the rest of the leg.
Hammer toes. As the big toe pushes into the second toe, it often forces that toe upward and out of its normal position, eventually leading to a hammer toe deformity. Research on lesser toe deformities notes that hammer toe is commonly associated with an elongated second ray or an existing bunion, since the crowding created by hallux valgus directly contributes to this secondary deformity.
Calluses and corns. With the toes crowded and rubbing against each other or against the inside of a shoe in new ways, thickened skin tends to develop at the new pressure points, both on top of the toes and between them.
Balance changes. The big toe plays a meaningful role in stability during walking, particularly during push-off. As that function is compromised, some people notice subtle changes in balance, especially on uneven surfaces.
Altered walking mechanics. This is one of the more clinically interesting downstream effects. A gait analysis study comparing women with bilateral hallux valgus to healthy controls found that patients shifted their center of pressure away from the affected joint and increased hip internal rotation to compensate, changing how force moves through the entire leg with every step.
Knee pain. That same gait research found the compensation pattern increases knee abductor moments, a measurement closely tied to medial knee loading and a known predictor of knee osteoarthritis progression. In plain terms, the body's workaround for bunion pain can quietly increase stress on the knee.
Hip pain. Because the compensation often involves increased hip rotation, some people develop hip discomfort as a downstream effect of years of altered gait, particularly if the bunion has gone unaddressed for a long time.
Lower back discomfort. The same chain of compensation that affects the knee and hip can extend further up, since gait changes rarely stay isolated to a single joint. Lower back discomfort is a less direct but plausible downstream consequence in long-standing, uncorrected cases.
Hammer Toes
How It Develops: The big toe crowds and pushes the second toe out of its natural position.
Why It Matters: Can create a secondary toe deformity that may require separate treatment.
Calluses and Corns
How It Develops: Friction increases as toes rub against each other or against the inside of shoes.
Why It Matters: Can become painful and may lead to skin breakdown if left untreated.
Balance Changes
How It Develops: Reduced big toe function affects stability during walking and push-off.
Why It Matters: May increase fall risk, particularly in older adults.
Altered Gait Mechanics
How It Develops: The body shifts weight and changes joint movement patterns to avoid bunion pain.
Why It Matters: Alters how force travels through the foot, ankle, knee, and hip during walking.
Knee Pain
How It Develops: Gait compensation can increase stress on the inner portion of the knee joint.
Why It Matters: Associated with increased medial knee loading and a higher risk of osteoarthritis progression.
Hip Pain
How It Develops: Increased hip rotation develops as the body compensates for altered foot mechanics.
Why It Matters: May contribute to chronic hip discomfort over time.
Lower Back Discomfort
How It Develops: Compensation patterns can travel up the kinetic chain from the foot to the spine.
Why It Matters: Long-term movement changes may contribute to lower back pain and stiffness.
Many people focus entirely on the toe itself and never connect a nagging knee or hip ache to a bunion they've had for years. If you're dealing with unexplained joint pain elsewhere in the leg and you also have a long-standing bunion, it's worth mentioning both to whoever is evaluating you, since they may be more connected than they appear.
See a doctor if your bunion causes increasing pain, makes walking difficult, no longer fits in regular shoes, starts overlapping with your second toe, or comes with persistent swelling or stiffness. These signs suggest the deformity is progressing faster than typical or that another issue, like arthritis, may be involved.
Most bunions don't require urgent attention, but certain signs mean it's worth getting a professional opinion rather than continuing to manage things on your own.
Increasing pain. If pain that used to be occasional or mild starts becoming frequent or intense, that's a sign the joint may be progressing faster than expected.
Difficulty walking. Any change in how you walk, especially if you notice yourself favoring the other foot or shortening your stride to avoid pain, is worth having evaluated.
Shoes no longer fitting. A rapid change in which shoes fit comfortably can indicate the bunion is advancing more quickly than a typical, slow progression.
Toe crossover. If the big toe starts to actually overlap with the second toe, this is a sign of more advanced deformity and is worth addressing before it progresses further.
Persistent swelling. Swelling that doesn't resolve with rest, ice, or time, especially if it's accompanied by warmth or redness, should be checked out to rule out infection or an inflammatory flare.
Signs of arthritis. Stiffness, grinding sensations in the joint, or pain that's present even at rest can indicate arthritis has developed alongside the bunion, which can change the treatment approach significantly.
If you're experiencing any of these, it's reasonable to schedule a visit with a podiatrist or orthopedic foot specialist rather than waiting to see if things improve on their own.
Big toe pain isn't always a bunion. Here's how to tell the difference.
Bunion
Location: Base of the big toe on the inside edge of the foot
Key Difference: Visible bony bump with the big toe gradually angling toward the second toe.
Gout
Location: Big toe joint, often affecting the same area as a bunion
Key Difference: Sudden, severe pain that frequently develops overnight and is accompanied by redness, warmth, and swelling.
Arthritis
Location: Big toe joint or multiple joints throughout the foot
Key Difference: Joint stiffness and aching pain, often worse in the morning, without the characteristic bunion bump or toe deviation.
Turf Toe
Location: Base of the big toe
Key Difference: Acute sports-related injury caused by hyperextension of the toe, typically resulting in sudden pain and swelling.
Sesamoiditis
Location: Underside of the big toe joint beneath the ball of the foot
Key Difference: Pain is felt underneath the foot rather than along the side of the joint and is usually worse during push-off while walking or running.
If your big toe pain came on suddenly and intensely, especially overnight, that pattern is more consistent with gout than a bunion. If pain is worse specifically under the joint rather than on the side, sesamoiditis is more likely. A bunion is identifiable mainly by its visible structural shift. If your discomfort doesn't match any of these patterns, our foot pain location guide can help you narrow down what's actually going on based on exactly where it hurts.
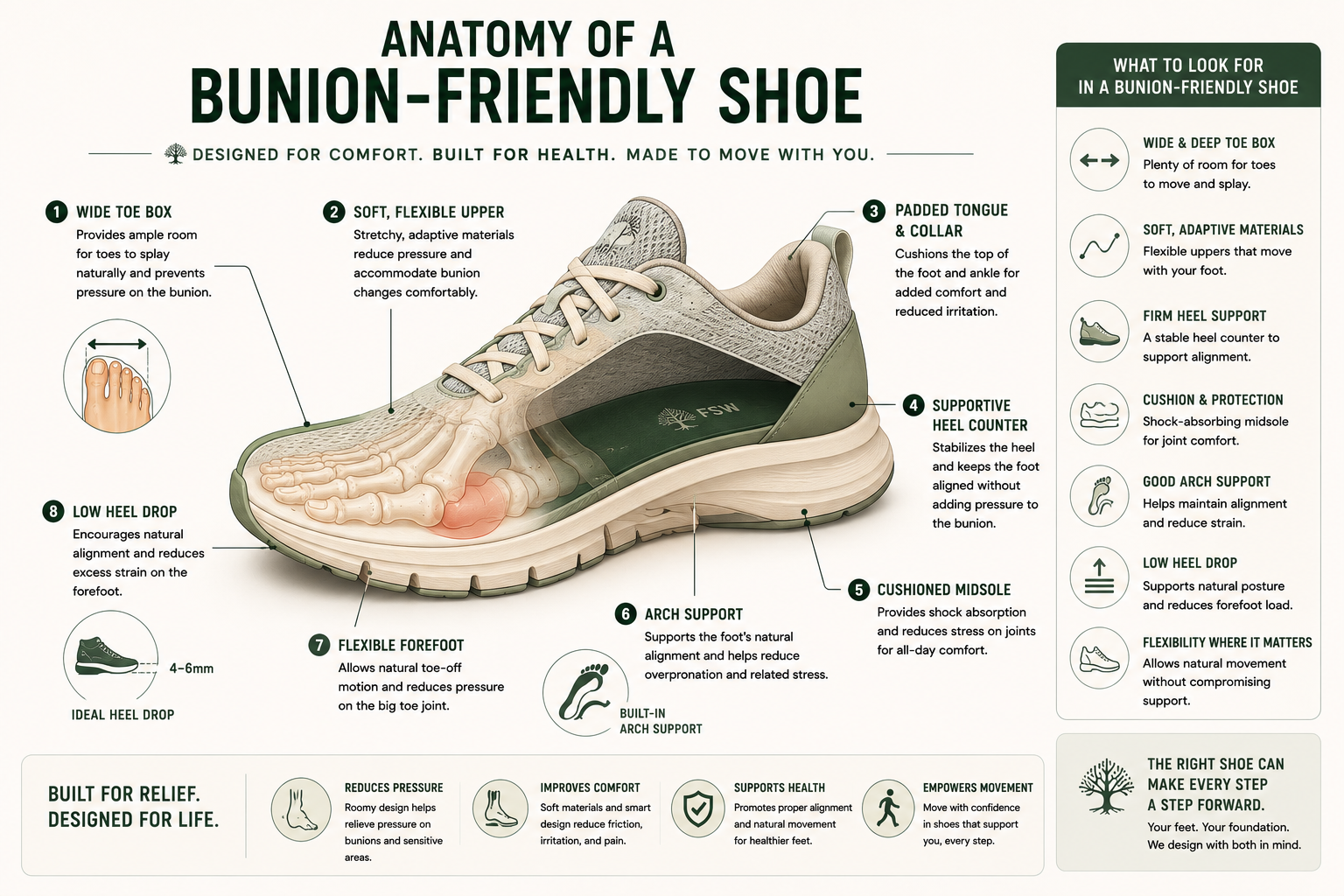
The best shoes for bunions have a wide, rounded toe box, soft and flexible uppers, a stable midsole, adequate arch support, and a low or flat heel. These features reduce pressure on the joint and slow how quickly the deformity progresses, while narrow, pointed, or high-heeled shoes do the opposite.
The right footwear is the single biggest lever you have for managing bunion pain day to day, and it's worth understanding exactly what to look for.
Wide toe boxes. This is the most important feature by far. A wide toe box gives the forefoot room to sit in its natural position instead of being squeezed into a narrower shape than the bones underneath it.
Rounded forefoot shape. Beyond just width, the actual shape of the front of the shoe matters. A rounded or anatomical forefoot shape follows the natural outline of a healthy foot rather than tapering to a point, which reduces pressure specifically at the bunion joint.
Soft uppers. The material directly over the bunion matters as much as the overall shape. Soft, flexible, stretchable uppers, often mesh or soft leather, flex around the bump instead of pressing directly into it the way stiff materials do.
Stable midsoles. A supportive, stable midsole helps control excess motion through the foot during walking, which reduces the repetitive stress placed on the big toe joint with every step.
Arch support. Since flat feet and overpronation are common contributors to bunion progression, adequate arch support helps address one of the underlying mechanical drivers rather than just managing the symptom.
Heel height considerations. Lower, more stable heels keep weight distributed more evenly across the foot. Higher heels shift weight forward onto the toes, increasing pressure directly on the bunion with every step.
Here's the same information condensed into a quick-reference table.
Wide Toe Box
Why It Helps: Allows the forefoot and toes to sit naturally without being squeezed into a narrower shape, reducing pressure on the bunion.
Rounded Forefoot
Why It Helps: Follows the natural shape of the foot and minimizes direct pressure on the big toe joint.
Soft Upper
Why It Helps: Flexes around the bunion rather than pressing against it, helping reduce friction and irritation.
Stable Midsole
Why It Helps: Controls excessive foot motion during walking, reducing repetitive stress placed on the bunion joint.
Arch Support
Why It Helps: Helps manage overpronation and supports proper foot mechanics, which may reduce strain on the big toe joint.
Low Heel
Why It Helps: Keeps body weight distributed more evenly across the foot instead of shifting excess pressure onto the forefoot and toes.
Narrow toe boxes. Anything that tapers and compresses the front of the foot directly worsens bunion pain and accelerates the inward pressure on the joint.
Pointed shoes. Pointed toe shapes are essentially a more extreme version of a narrow toe box, forcing the toes into a shape that doesn't match the foot's actual structure.
High heels. Beyond the heel height itself, most high heels also combine a narrow toe box with an elevated heel, compounding the pressure on the forefoot.
Excessively compressive uppers. Stiff materials like rigid leather or synthetic overlays that don't flex around the bunion create constant friction and pressure exactly where you don't want it.
[ILLUSTRATION: Bunion-friendly shoe anatomy.]
If you're working through which specific shoes fit these criteria, our best shoes for bunions roundup breaks down tested options by category, and many of the same principles carry over if you're also managing flat feet alongside a bunion. Our wide toe box shoes guide goes deeper on toe box shape specifically if that's your main priority. These same six features are also the foundation for choosing walking shoes or running shoes if you're dealing with a bunion and staying active, since the joint takes on more repetitive load during exercise than it does during a normal day on your feet.
You can't fully prevent a bunion if you're genetically predisposed to one, but you can meaningfully slow how fast it develops and how much it affects you.
Footwear. Choose shoes with a wide toe box that allows your toes to sit naturally without compression. Save narrow or high-heeled shoes for occasional wear rather than daily use.
Foot strength. Regular foot-specific strengthening, like the exercises above, helps the muscles around the joint provide better support against the forces pulling it out of alignment. Our foot strengthening exercises guide covers additional routines if you want to build this into a broader foot health habit.
Mobility. Keeping the big toe joint mobile through regular stretching helps maintain function and may reduce compensatory strain elsewhere in the foot.
Managing flat feet. If overpronation is part of your foot mechanics, addressing it with proper arch support or orthotics reduces one of the major mechanical drivers of bunion progression. Check out our overpronation explained guide for a deeper look at how this pattern develops and what to do about it.
Activity considerations. High-impact repetitive activities in unsupportive footwear can accelerate joint stress. This doesn't mean avoiding exercise. It means pairing activity with appropriate footwear.
There's a lot of misinformation floating around about bunions, much of it driven by products promising results the science doesn't support. Here's a quick reality check.
Myth: Bunions are just a bump.
Fact: A bunion is a structural shift in the bones, ligaments, and tendons of the big toe joint. The visible bump is simply the outward appearance of that underlying deformity.
Myth: Tight shoes cause all bunions.
Fact: Genetics and foot structure are the primary drivers of bunion development. Tight or narrow shoes can accelerate progression and increase discomfort, but they are rarely the sole cause.
Myth: Exercises can reverse a bunion.
Fact: Exercises can improve foot strength, mobility, and symptom management, but they cannot move the bones back into their original position. Surgery is the only treatment that can structurally correct a bunion.
Myth: Every bunion eventually needs surgery.
Fact: Many people successfully manage bunions for life with proper footwear, activity modifications, orthotics, and strengthening exercises. Surgery is typically reserved for persistent pain or functional limitations.
Myth: Bunion surgery is cosmetic.
Fact: The primary goal of bunion surgery is to reduce pain, improve function, and restore joint alignment. Surgical decisions are usually based on symptoms and quality of life, not appearance alone.
Can bunions go away on their own?
No. Bunions are progressive structural changes in the joint, and they don't resolve without intervention. In rare cases, very mild bunions may stay stable for years without worsening, but the deformity itself won't reverse on its own.
What is the main cause of bunions?
Genetics is the leading cause of bunions, with research showing the condition is highly heritable and tends to run strongly in families. Foot structure, ligament laxity, and biomechanical factors like flat feet build on that genetic foundation. Footwear, particularly narrow or pointed shoes, doesn't cause bunions on its own but can speed up progression and increase pain in people who are already predisposed.
Do bunions get worse with age?
Yes, in most cases. Bunions are progressive, meaning the structural deviation tends to increase over time rather than staying static. Population data shows prevalence climbing from roughly 23% in adults under 65 to around 36% in adults over 65, reflecting both new cases developing and existing bunions advancing further with cumulative years of joint stress.
Do toe spacers work?
Toe spacers can reduce pain and pressure while worn and may help slow progression in early-stage bunions. They don't provide a permanent correction, and any realignment they create disappears once you take them off.
Can running make bunions worse?
Running itself doesn't cause bunions, but running in narrow or poorly fitted shoes can accelerate irritation and progression in someone who already has a bunion or a predisposition to one. Proper footwear matters more for runners than for most other activities.
Are bunions hereditary?
Yes, in large part. Foot structure, ligament laxity, and joint alignment are all inherited traits, and research consistently shows bunions running in families independent of shared footwear habits.
What shoes are best for bunions?
Shoes with a wide, rounded toe box, soft uppers that don't press on the bump, low or no heel, and adequate arch support tend to work best. Avoid pointed toes and high heels, which compress the forefoot directly into the area causing pain.
Can bunions cause knee or hip pain?
Indirectly, yes. A bunion can change your gait pattern as you shift weight away from the painful joint, and that altered mechanics can place extra stress on the knees, hips, or lower back over time.
Do all bunions require surgery?
No. Most bunions are managed successfully without surgery, especially when caught early and paired with proper footwear and strengthening. Surgery is reserved for cases where pain or function is significantly impaired despite conservative treatment.
How fast do bunions progress?
Progression speed varies widely and depends on genetics, foot structure, and footwear habits. Some bunions stay mild for decades, while others advance from mild to moderate within just a few years, especially when an underlying driver like uncontrolled flat feet goes unaddressed. There's no fixed timeline, which is why monitoring changes over time matters more than comparing to a general average.
Can bunions return after surgery?
Yes, recurrence is possible, particularly if the underlying biomechanical cause, like overpronation or an unstable first ray, isn't addressed alongside the surgical correction. Choosing the right procedure for the severity of the original deformity also plays a significant role in long-term surgical success.
Do toe spacers prevent bunions?
Toe spacers aren't well supported as a true prevention tool for people who haven't developed a bunion yet. Their main evidence base is for symptom relief and possibly slowing progression in people who already have early-stage hallux valgus, not for preventing the condition from starting in someone with no existing deformity.
Can barefoot shoes help bunions?
Barefoot and wide toe box minimalist shoes can help in the sense that they avoid compressing the forefoot, which removes one of the accelerating factors in bunion progression. They don't reverse existing deformity, and a sudden switch to minimalist footwear without an adjustment period can create its own strain elsewhere in the foot, so transitioning gradually matters.
Can a bunion cause numbness?
Yes, in some cases. As the joint shifts and surrounding tissue becomes inflamed or compressed, nearby nerves can become irritated, leading to numbness or a tingling sensation, most often along the side or top of the big toe. Persistent numbness is worth mentioning to a doctor, since it can also signal nerve compression that benefits from specific treatment.
Can bunions be prevented?
Not entirely if you're genetically predisposed, since heredity is the largest single factor in who develops hallux valgus. What you can do is meaningfully slow how quickly a bunion develops and how much it affects you, primarily through wide toe box footwear, foot strengthening, and addressing flat feet or overpronation if they're present.
Bunions rarely exist in isolation. Here are a few conditions worth knowing about if you're dealing with one.
Flat Feet. A collapsed or low arch that changes how weight moves through the foot, often setting the stage for bunion development.
Overpronation. Excessive inward rolling of the foot during walking, frequently linked to flat feet and a major mechanical driver behind bunion progression.
Hammer Toes. A bending deformity of the smaller toes, often caused by the crowding a bunion creates as the big toe pushes into the second toe.
Tailor's Bunion. A similar bony bump that forms at the base of the little toe instead of the big toe, driven by the same kind of metatarsal misalignment on the opposite side of the foot.
Plantar Fasciitis. Inflammation of the thick band of tissue running along the bottom of the foot, causing heel pain that's unrelated to bunions but common in the same population of people on their feet all day.
Morton's Neuroma. A thickening of nerve tissue between the third and fourth toes, causing burning pain or numbness in the forefoot that's sometimes mistaken for bunion-related discomfort.
This article is for educational purposes and is not a substitute for professional medical advice. If you're experiencing significant foot pain or considering treatment options, consult a podiatrist or orthopedic specialist for an evaluation specific to your condition.
Nix, S., Smith, M., & Vicenzino, B. (2010). Prevalence of hallux valgus in the general population: A systematic review and meta-analysis. Journal of Foot and Ankle Research, 3, 21.
Hannan, M. T., Menz, H. B., Jordan, J. M., Cupples, L. A., Cheng, C. H., & Hsu, Y. H. (2013). High heritability of hallux valgus and lesser toe deformities in adult men and women. Arthritis Care & Research, 65(9), 1515 to 1521.
Meh, S. G., Pešič, M., & Kozinc, Ž. (2026). Effects of foot strengthening exercises with or without a toe spacer on hallux alignment, foot mobility, and balance: A randomized controlled trial. Applied Sciences, 16(7), 3163. Conducted in healthy adults without diagnosed hallux valgus.
Shih, K.-S., Chien, H.-L., Lu, T.-W., Chang, C.-F., & Kuo, C.-C. (2014). Gait changes in individuals with bilateral hallux valgus reduce first metatarsophalangeal loading but increase knee abductor moments. Gait & Posture, 40(1), 38 to 42. Compared gait kinematics in twelve women with bilateral hallux valgus to healthy controls during level walking.
American Academy of Orthopaedic Surgeons (AAOS). Patient-facing guidance on bunion surgical outcomes and recovery expectations.
American Orthopaedic Foot & Ankle Society (AOFAS). Clinical guidance identifying footwear modification as a first-line conservative intervention for symptomatic hallux valgus.