Plantar fasciitis is one of the most common causes of heel pain. Learn the symptoms, causes, treatment options, and exercises that can help you recover and stay pain-free.
At first, most people assume it's just a sore heel. Maybe you walked too much yesterday. Maybe your shoes are getting old. Then the pain keeps showing up every morning and suddenly you're limping to the coffee maker wondering what happened.
That sharp, stabbing sensation with your first few steps out of bed is one of the most recognizable symptoms in all of orthopedic medicine, and it has a name: plantar fasciitis.
Plantar fasciitis is responsible for roughly 1 million doctor visits per year in the United States alone, according to research published in the Journal of Foot and Ankle Surgery. It touches every kind of person: marathon runners, nurses pulling 12-hour shifts, teachers on hard classroom floors, and people who simply stood too long at the wrong time in the wrong shoes.
The good news is that this is one of the most well-understood foot conditions in orthopedic medicine. We know what causes it, why it behaves the way it does, and what actually resolves it. This guide covers all of it.
Plantar fasciitis is irritation and degeneration of the plantar fascia, a thick band of tissue that runs along the bottom of the foot from the heel to the toes. It is the most common cause of heel pain in adults and is known for causing sharp, stabbing pain with the first steps in the morning.
Historically, plantar fasciitis was thought to be purely inflammatory. More recent research suggests many chronic cases involve degeneration of the fascia tissue itself: breakdown of collagen, loss of normal fibrous structure, rather than active inflammation. This is why some clinicians now use the term plantar fasciosis to describe longer-standing cases. The distinction matters for treatment. Anti-inflammatory approaches alone are often insufficient once degeneration has taken hold.
Let's start with the name itself, because it tells you almost everything about the condition, and also about where the science has moved beyond it.
The plantar surface of your foot is the bottom, the side that faces the ground when you stand. The fascia is a type of dense connective tissue found throughout your body. Think of it like cling film made of collagen: tough, fibrous, and designed to wrap and protect structures while helping them move. And -itis is a medical suffix that means irritation or inflammation.
So plantar fasciitis, at its most literal, means irritation of the connective tissue on the bottom of your foot. The name stuck, but our understanding of what's actually happening in the tissue has evolved considerably.
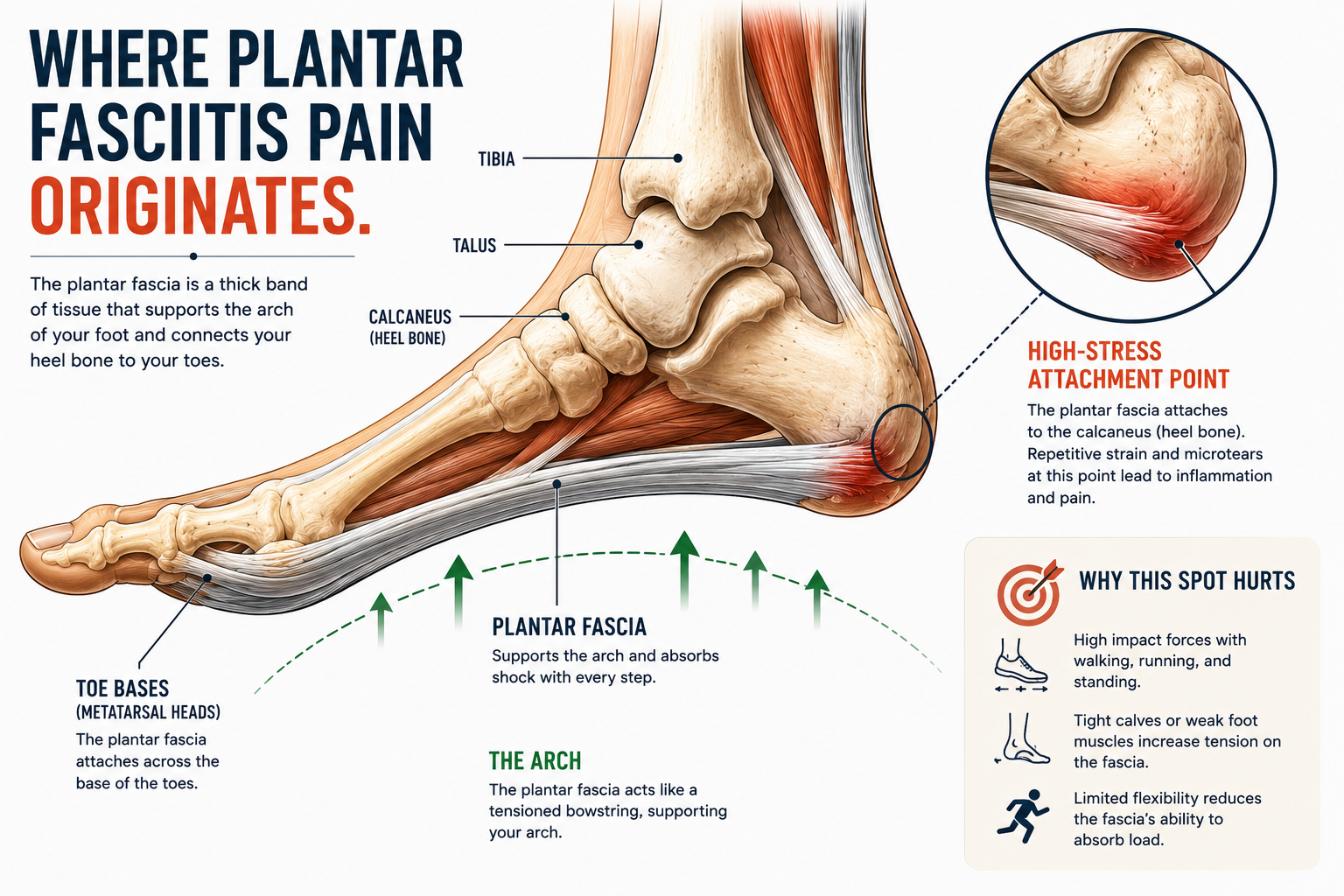
The plantar fascia itself is a thick, triangular band of tissue that originates at your heel bone (the calcaneus) and fans outward toward the base of your five toes. Its primary job is structural. It acts like a tension cable that holds the arch of your foot together, absorbs the mechanical shock of each step, and helps your foot spring forward efficiently when you push off the ground.
Researchers often describe this mechanism as the "windlass effect," a term borrowed from the mechanics of pulling a ship's anchor. When your toes bend upward during walking, the plantar fascia tightens and compresses the arch, storing and releasing energy like a spring. It's an elegant, load-bearing system that works silently and seamlessly in a healthy foot.
The problem starts when that load exceeds what the tissue can handle.
When the plantar fascia is subjected to repeated stress, from long hours on your feet, inadequate footwear, tight calf muscles, or a sudden increase in activity, it develops small tears at the microtissue level. The area where the fascia attaches to the heel bone is particularly vulnerable. That attachment point takes the most strain with every step, and over time, the repeated micro-tearing disrupts the normal collagen structure of the tissue. In early, acute cases some true inflammation is present. In longer-standing cases, research increasingly shows that the dominant process is degeneration: collagen breakdown, disorganized fiber structure, and a loss of the tissue's normal load-bearing architecture. This is why corticosteroid injections, which target inflammation, often provide only temporary relief in chronic cases, while tissue-remodeling approaches like stretching, strengthening, and shockwave therapy tend to produce more durable results.
Your foot is more architecturally complex than most people give it credit for. It contains 26 bones, 33 joints, and over 100 muscles, tendons, and ligaments, all working together in a space smaller than a sheet of paper.
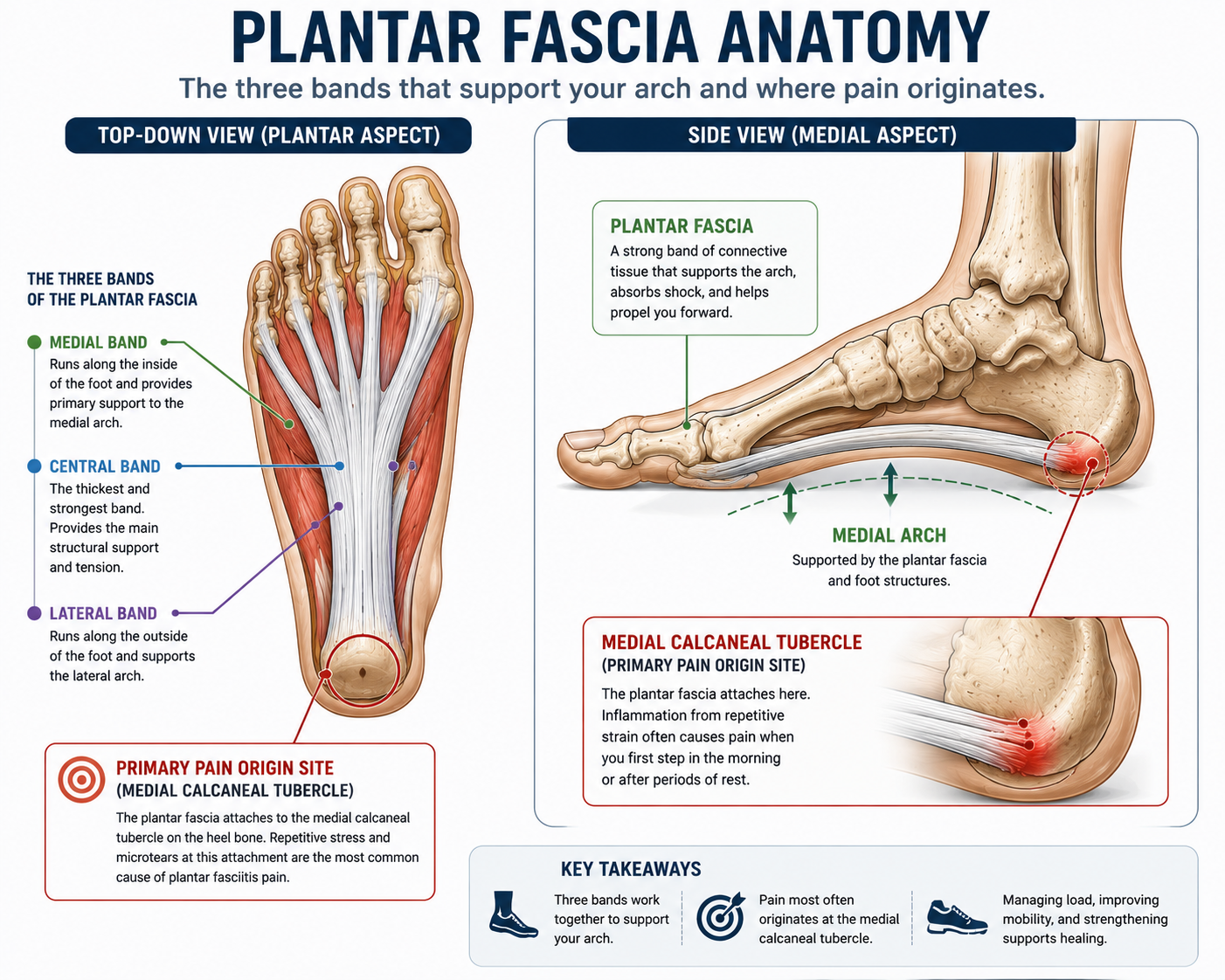
The plantar fascia lives on the underside of this structure, running along the entire length of the foot. It has three distinct sections, or bands: a central band, which is the thickest and most commonly involved in plantar fasciitis; a medial band along the inner edge of the arch; and a lateral band along the outer edge.
When plantar fasciitis develops, pain is almost always concentrated at the medial calcaneal tubercle, the bony bump on the inner side of the heel where the central band attaches. This is the point of maximum mechanical stress, and it's typically where you will feel the sharpest pain when you press into your heel with your thumb.
Pain can also radiate along the arch toward the ball of the foot in more significant cases, though the heel origin remains the most common presentation.
Plantar fasciitis doesn't usually have a single cause. In most cases, it results from a combination of factors that gradually overwhelm the tissue's capacity to recover. Understanding these causes is the first step toward addressing the actual problem rather than just managing the pain.
The plantar fascia is designed to handle load, but it has limits. When you subject it to the same mechanical stress day after day without adequate recovery time, the micro-tears accumulate faster than the tissue can repair itself. This is why plantar fasciitis is especially common in long-distance runners, retail and healthcare workers, and teachers. The issue isn't any single step. It's the cumulative volume.
A 2014 study published in Clinical Biomechanics found that plantar fascia strain peaks at approximately 9.5% of the fascia's length during normal walking, a significant load that multiplies across thousands of steps per day.
Concrete, tile, and hardwood floors offer no energy return. Every step sends the full force of impact straight up through your heel. Over the course of an eight-hour shift, that adds up to a substantial amount of cumulative stress on the fascia and its attachment point. This is one of the primary reasons plantar fasciitis is so prevalent among healthcare workers. Nurses report this condition at rates significantly higher than the general population.
This connection surprises most people, but the research is consistent: limited dorsiflexion, which is the ability to flex your foot upward toward your shin, is one of the strongest independent risk factors for plantar fasciitis.
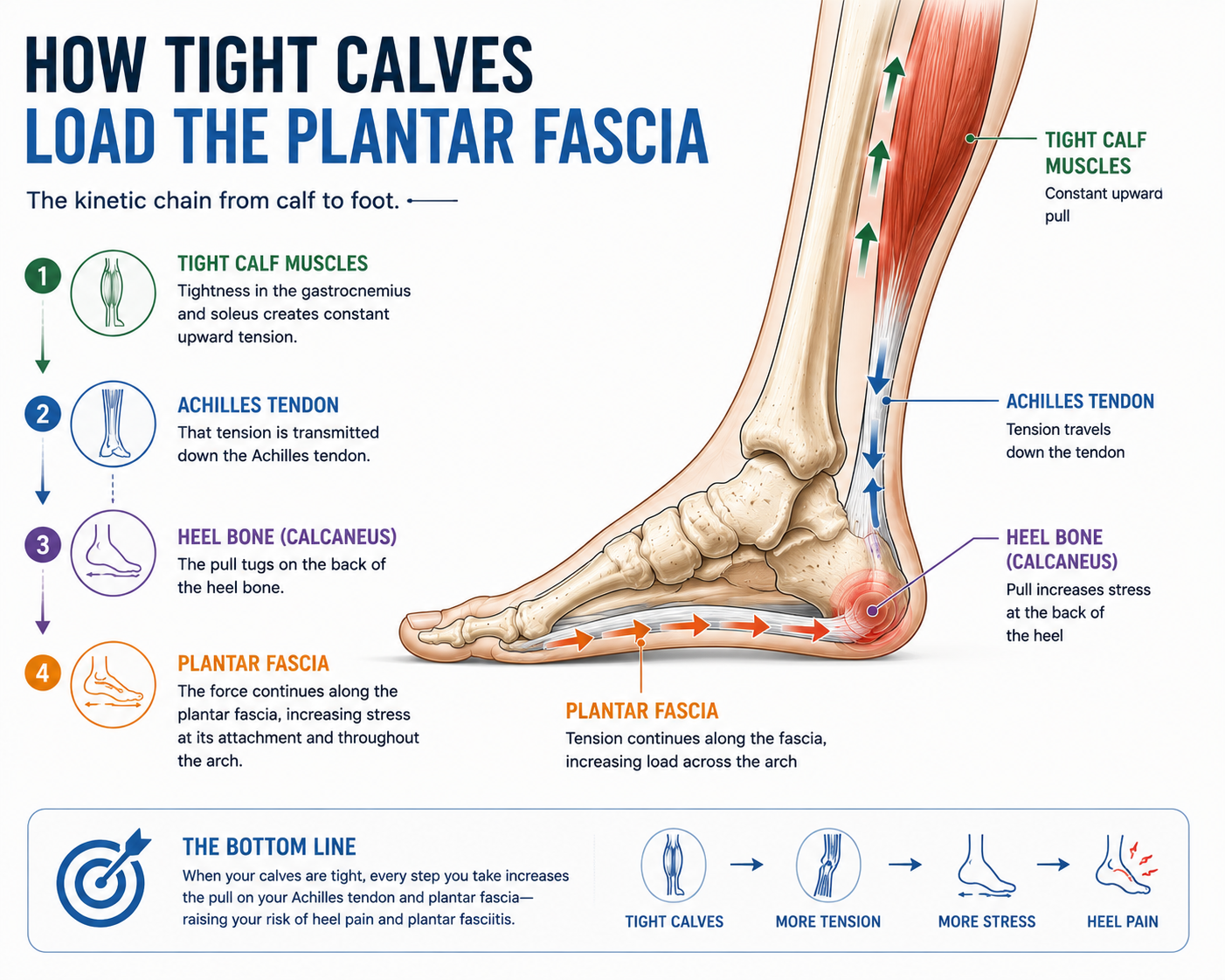
Here's why. Your calf muscles (the gastrocnemius and soleus) connect to your heel bone via the Achilles tendon, the thick cord you can feel running up the back of your ankle. When these muscles are tight, they pull the heel bone backward and upward during walking, which increases tension on the plantar fascia below. Tightness at the back of the leg travels directly into strain at the bottom of the foot. It's a chain reaction most people never see coming.
A systematic review published in the Journal of Orthopaedic and Sports Physical Therapy found that patients with plantar fasciitis had significantly less ankle dorsiflexion range of motion compared to pain-free controls. Stretching the calf and Achilles is therefore not just supportive treatment. It's addressing a root cause.
Tight calves are one of the most overlooked drivers of plantar fasciitis. For a deeper breakdown of exactly how this works and what to do about it, read our full guide: How Tight Calves Cause Foot Pain.
Overpronation is a word you'll hear often in discussions of foot health. It describes the tendency of the foot to roll inward excessively during the walking or running cycle. Pronation itself is a normal part of how the foot absorbs impact. It's only "over"-pronation when the degree becomes excessive.
When the foot overpronates, the arch collapses more than it should with each step. This repetitive collapse stretches the plantar fascia beyond its comfortable working range, particularly at the heel attachment. Over time, this sustained over-stretching creates the same pattern of micro-tearing and tissue breakdown seen in other presentations of the condition.
Flat feet are often, though not always, associated with overpronation. Internal links: → See Flat Feet and Plantar Fasciitis
On the opposite end of the spectrum, high arches create a different mechanical problem. A very high arch is inherently rigid. It doesn't pronate enough, which means it absorbs very little shock. Instead, ground reaction forces concentrate in a small area at the heel and ball of the foot rather than being distributed across the entire foot structure. That concentrated loading increases stress on the plantar fascia significantly.
Flat, thin-soled shoes like flip flops, ballet flats, and minimalist sneakers worn by people who aren't ready for them provide almost no cushioning or arch support. When you stand or walk in these shoes for hours, your plantar fascia absorbs mechanical load it was never designed to carry alone.
Conversely, extremely high heels create a different problem. They place the foot in a sustained position of plantarflexion (pointing downward), which shortens the calf muscles over time and increases tension on the plantar fascia. → See How Footwear Affects Plantar Fasciitis (Section 10)
Starting a new training program, returning to exercise after a long break, or significantly increasing your weekly mileage without adequate build-up time are common triggers. The plantar fascia, like any other connective tissue, needs time to adapt to new loads. Push it too fast and the micro-damage outpaces the repair process.
The symptom profile of plantar fasciitis is distinctive enough that many clinicians can diagnose it from description alone before ever examining the foot.
The classic presentation includes:
Symptom Summary Box
Typical Timing: First steps in the morning.
This is the hallmark symptom of plantar fasciitis. Many people describe it as feeling like stepping on a nail or sharp rock when they first get out of bed.
Typical Timing: After prolonged sitting or periods of rest.
The plantar fascia runs the entire length of the arch, so irritation can create a feeling of tightness or pulling through the middle of the foot.
Typical Timing: During or after activity.
Many people notice that the pain improves after a few minutes of walking, only to return later in the day after prolonged standing, walking, or exercise.
Typical Timing: When pressure is applied directly to the area.
Pressing firmly on the inside-bottom portion of the heel often reproduces the pain and is one of the most useful clues during a physical examination.
Typical Timing: Upon waking or after long periods of inactivity.
The plantar fascia tightens while resting, which is why the foot often feels stiff and uncomfortable before it has had a chance to warm up and move.
What plantar fasciitis typically does NOT feel like:
Numbness, tingling, or burning that radiates up the leg suggests a nerve component, rather than or in addition to plantar fascia involvement, and warrants professional evaluation. Swelling that is visually obvious or pain that is equally severe at rest as during activity is also worth having assessed.
Before we go deeper, run through this quickly. Check any that apply to your experience:
If you checked three or more of these, plantar fasciitis is the most likely explanation. If you checked all six, the clinical picture is very clear. That said, this is not a substitute for professional diagnosis, particularly if you have numbness, tingling, or significant swelling alongside the pain, which can indicate other conditions. We cover the diagnostic process fully in Section 7.
Location is one of the clearest diagnostic indicators for plantar fasciitis, and it's worth being specific because a lot of foot pain gets lumped together incorrectly.
The heel is where most people feel it, specifically the inner-bottom surface of the heel, right where the plantar fascia attaches to the calcaneus bone. Press your thumb firmly into that spot right now. If that produces a sharp, familiar pain, you've found the source.
The arch becomes involved as the condition progresses or in more severe cases. The pain may radiate from the heel along the inner edge of the arch toward the midfoot. This is still plantar fascia involvement since the fascia runs the full length of the arch, but arch-dominant pain can sometimes indicate a different presentation that warrants clinical evaluation.
The toes are rarely involved. If pain or numbness is concentrated at the toes or ball of the foot, the problem is more likely metatarsalgia, a neuroma, or a nerve-related issue rather than plantar fasciitis.
One foot or both? Plantar fasciitis most commonly affects one foot at a time, typically the dominant side or the foot that bears more load due to posture asymmetries. Bilateral plantar fasciitis, meaning both feet simultaneously, does occur, most often in people with significant overpronation or those who increased activity volume rapidly. If both feet are severely affected at the same time, it's worth having your gait assessed.
The honest answer is that for most straightforward cases, the diagnosis is clinical, meaning it's based on your history and a physical exam, not a scan. The symptom pattern of plantar fasciitis is distinctive enough that an experienced clinician can identify it without imaging in the majority of cases.
Your clinician will assess tenderness at the medial calcaneal tubercle (that inner heel attachment point), test your ankle dorsiflexion range of motion, check for tightness in the calf and Achilles complex, and observe your foot arch and gait. This hands-on assessment provides more useful information for treatment planning than most imaging can.
When imaging is needed, diagnostic ultrasound is the first-line choice. It can visualize the plantar fascia directly, measuring its thickness (greater than 4mm is considered abnormal), identifying tears, and detecting degenerative changes in the tissue structure. It's inexpensive, real-time, and doesn't involve radiation. Some sports medicine clinics use ultrasound routinely for plantar fasciitis confirmation and to guide injection therapy when needed.
X-rays don't show soft tissue, so they can't directly image the plantar fascia. What they do show is bone, specifically the presence of a heel spur (a calcium deposit at the plantar fascia attachment). As discussed in the conditions comparison section, heel spurs frequently coexist with plantar fasciitis but are often not the primary source of pain. X-rays are useful mainly to rule out stress fractures or other bony pathology that could be causing heel pain.
MRI is rarely necessary for a standard plantar fasciitis diagnosis but may be ordered in atypical presentations, when the diagnosis is genuinely unclear, or when conservative treatment has failed and a clinician wants to assess for plantar fascia tears, soft tissue masses, or other structural issues. It's a powerful diagnostic tool. It simply isn't needed in most routine cases.
The bottom line: if your symptoms fit the classic pattern, you likely don't need imaging before starting treatment. If your pain is atypical, worsening rapidly, or not responding to standard care, imaging helps refine the picture significantly.
The signature morning heel pain of plantar fasciitis is not a coincidence. It has a clear physiological explanation, and once you understand it, you can actually use that knowledge to reduce the pain.
While you sleep, your feet naturally settle into a position of plantarflexion, toes pointed slightly downward, ankle relaxed. In this position, the plantar fascia shortens and sits in a relatively compressed, resting state. Any micro-tears that occurred during the previous day begin a low-level repair process overnight.
The moment you stand up and take your first steps, the plantar fascia is suddenly and forcefully stretched from that shortened resting position to its fully loaded working position. This rapid stretch disrupts the fragile repair tissue that has been forming overnight and re-irritates the damaged zone at the heel attachment. That is the characteristic sharp, gasping pain that plantar fasciitis sufferers know all too well.
After a few minutes of walking, the tissue warms up, the repair tissue becomes more pliable, and the surrounding structures loosen slightly. Pain often diminishes, sometimes significantly, during this period. This temporary relief is real, but it can be misleading. The underlying condition is not resolving. The tissue is simply accommodating to the load.

This is also why night splints are one of the more evidence-supported treatments for plantar fasciitis. These devices hold the foot in a slightly dorsiflexed position during sleep, which prevents the fascia from shortening overnight and significantly reduces that first-step pain. → See Treatment Section
Heel pain is not always plantar fasciitis. Several other conditions produce similar or overlapping symptoms, and getting the distinction right matters for treatment.
Primary Pain Location: Inner heel and bottom of the foot
Key Differentiator: Pain is typically worst with the first steps in the morning, improves after walking for a short period, and then often returns after prolonged standing or activity.
Primary Pain Location: Back of the heel and lower Achilles tendon
Key Differentiator: Pain is located behind the ankle rather than underneath the foot and is often aggravated by running, jumping, or climbing stairs.
Primary Pain Location: Bottom of the heel
Key Differentiator: Often found alongside plantar fasciitis. Many people have heel spurs without pain, meaning the spur itself is rarely the primary cause of symptoms.
Primary Pain Location: Ball of the foot, just behind the toes
Key Differentiator: Pain is concentrated in the front of the foot rather than the heel and often feels like walking on a pebble or bruised tissue.
Primary Pain Location: Diffuse pain throughout the entire foot
Key Differentiator: Usually resolves with rest and does not create the sharp, localized heel tenderness that is common with plantar fasciitis.
Primary Pain Location: Inner heel
Key Differentiator: Often produces burning, tingling, numbness, or nerve-like symptoms in addition to heel pain.
A note on heel spurs: they show up on X-rays of plantar fasciitis patients frequently enough that people often assume the spur is the problem. Research tells a different story. Studies have found heel spurs in a significant percentage of people with no heel pain at all. They're typically a downstream effect of chronic plantar fascia tension rather than an independent cause of pain. Treating the fascia, not the spur, is the appropriate approach in the vast majority of cases.
→ For more detail: Heel Pain vs. Plantar Fasciitis | Achilles Tendinitis vs. Plantar Fasciitis
Your shoes are not passive containers for your feet. They actively shape how force is distributed with every step you take. The wrong pair doesn't just fail to help. It can actively perpetuate or worsen the condition. Choosing the right footwear is one of the highest-impact changes you can make for plantar fasciitis recovery. See our complete guide to the Best Shoes for Plantar Fasciitis for specific brand and model recommendations vetted for this condition.
Here are the four footwear variables that matter most:
Adequate midsole cushioning absorbs ground reaction force before it reaches the plantar fascia. This is particularly important on hard surfaces. Shoes with worn-out midsoles, those that have lost their compression-absorption capacity, offer significantly less protection than they appear to from the outside. The outsole may look fine while the midsole has fully compacted. If your shoes are more than 12 months old and you're on your feet heavily, the cushioning has likely degraded.
Proper arch support reduces the degree to which the plantar fascia must act as the primary structural support for your arch. A contoured footbed that matches your arch shape distributes load across the entire plantar surface rather than concentrating it at the heel attachment point. This is why supportive shoes tend to feel immediately more comfortable for plantar fasciitis sufferers. They're sharing the mechanical load.
This one is underappreciated. A narrow toe box compresses the forefoot and forces the toes into an unnatural position, particularly the big toe, which is crowded inward (a condition called hallux valgus when severe). The big toe's ability to extend freely during the push-off phase of walking is directly tied to plantar fascia tension via the windlass mechanism described earlier. Restricting that extension increases strain on the fascia throughout the gait cycle. A wider toe box allows natural splay and reduces this load. → See Wide Toe Box Shoes Explained
Heel drop refers to the height difference between the heel and the forefoot in a shoe. A traditional running shoe might have a 10–12mm heel drop. A zero-drop shoe sits perfectly level. Heel drop matters for plantar fasciitis because a higher heel passively shortens the calf and Achilles, which increases plantar fascia tension. Transitioning to lower-drop or zero-drop footwear can be beneficial long-term, but must be done very gradually to avoid overloading tissue that isn't yet conditioned for it. → See Zero Drop Shoes for Plantar Fasciitis
→ Ready for specific recommendations? See Best Shoes for Plantar Fasciitis | Best Walking Shoes for Heel Pain | Best Shoes for Nurses with Plantar Fasciitis
The research on plantar fasciitis treatment is more robust than for many orthopedic conditions. Here's what the evidence actually supports, ranked from most foundational to most interventional.
This is the single most well-supported conservative treatment in the literature. A landmark study by DiGiovanni et al. published in the Journal of Bone and Joint Surgery demonstrated that Achilles tendon stretching produced significant improvement in pain and function in plantar fasciitis patients. The mechanism is direct: releasing tension in the calf-Achilles complex reduces the pulling force on the plantar fascia.
The protocol that has the strongest evidence:
→ See 7-Day Plantar Fasciitis Stretching Schedule for a full structured program | See How Tight Calves Cause Foot Pain
Equally important is stretching the fascia itself. Research by Barry et al. found that plantar-fascia-specific stretching produced superior outcomes compared to Achilles stretching alone in some patient populations.
The most effective technique: Before getting out of bed in the morning, before that first step, sit up and cross your affected foot over your opposite knee. Grip your toes and pull them back toward your shin until you feel a stretch along the arch and bottom of your foot. Hold 20–30 seconds. Repeat 3 times. Doing this before weight-bearing means you're gently lengthening the fascia before it gets suddenly loaded, which significantly reduces that first-step pain.
Stretching addresses tension. Strengthening addresses the root cause of why that tension is there. Weak intrinsic foot muscles, the small muscles that live inside the foot itself rather than in the leg, place disproportionate load on passive structures like the plantar fascia. Training these muscles builds an active support system that supplements the fascia's work. → See Section 12: Foot Strength for specific exercises
This doesn't mean stopping activity entirely. It means reducing the specific loads that aggravate the condition while maintaining overall fitness. Swapping pavement running for pool running or cycling maintains cardiovascular conditioning while giving the plantar fascia a relative rest. Complete immobility is rarely indicated and can actually delay recovery by reducing blood flow to the tissue.
Supportive sandals and slides worn around the house, rather than walking barefoot on hard floors, maintain arch support even during off-hours. Barefoot walking on hard surfaces is one of the most common aggravating factors that people overlook simply because it happens at home. Brands like Oofos specifically engineer their recovery footwear around reducing plantar fascia load, and the biomechanical evidence for this category is growing. → See Best Recovery Footwear for Plantar Fasciitis
A skilled physical therapist brings tools beyond what home treatment can offer: manual therapy to address joint mobility restrictions in the ankle and midfoot, dry needling to address trigger points in the calf and foot, gait retraining, and individualized exercise programming. For persistent cases, PT is a highly cost-effective intervention relative to more invasive options.
Custom orthotics are effective for addressing specific biomechanical contributors, particularly overpronation and high arches. A well-designed orthotic supports the arch, offloads the plantar fascia attachment, and corrects the foot's load-bearing alignment. Over-the-counter options like Superfeet or Powerstep work for many people and cost a fraction of custom devices. Custom orthotics are most appropriate when biomechanical issues are significant and off-the-shelf options haven't provided sufficient relief.
As discussed in the morning pain section, night splints hold the ankle at a neutral or slightly dorsiflexed angle during sleep, preventing the fascia from shortening overnight. Clinical trials show consistent improvement in first-step pain and overall symptoms with regular use. They take some getting used to, but for people whose morning pain is particularly severe, the evidence is strong.
When conservative measures have been consistently applied for 3–6 months without adequate resolution, additional options exist:
Modern footwear has done an extraordinary job of cushioning and supporting the foot, and in doing so, it has quietly allowed the foot's own muscles to weaken from underuse.
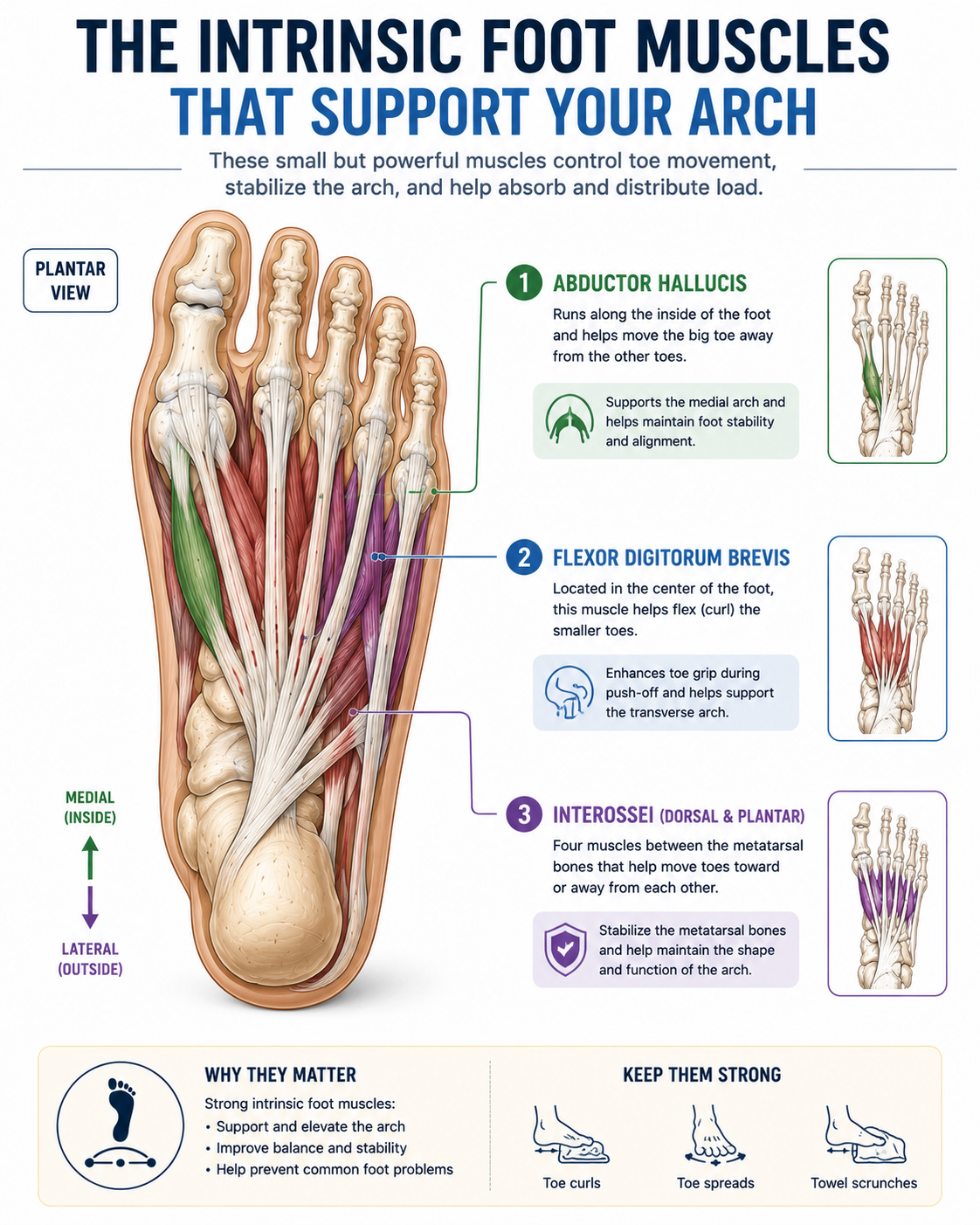
Your foot has two categories of muscles. Extrinsic muscles originate in the lower leg and send tendons down into the foot. These control larger movements like ankle flexion and extension. Intrinsic muscles live entirely within the foot itself, and their job is to control the fine architecture of the arch, stabilize the toes, and actively support the plantar fascia during loading.
When the intrinsic muscles are weak, the plantar fascia must carry a disproportionate share of the load. It's the structural equivalent of removing the load-bearing walls from a building and expecting the foundation alone to hold everything up. Over time, that foundation fails.
Research published in Physical Therapy in Sport has demonstrated that intrinsic foot muscle training significantly reduces plantar fasciitis symptoms and improves foot function, and the improvements are durable. They persist because they address the underlying weakness rather than simply compensating for it.
Three exercises with the strongest evidence base for plantar fasciitis:
This is the gold standard for intrinsic foot muscle activation. Sit in a chair with your foot flat on the floor. Without curling your toes, try to shorten the foot by drawing the ball of your foot toward your heel, which domes the arch upward. Hold 5–10 seconds, release, repeat 10 times per foot. This directly activates the abductor hallucis and flexor digitorum brevis, the primary intrinsic muscles that support the medial arch.
This exercise is deceptively simple. Most people find it extremely difficult at first because their intrinsic foot muscles are essentially untrained. That difficulty is itself diagnostic.
Place a small towel flat on the floor. Using only your toes, without lifting your heel, scrunch the towel toward you. This exercises the flexor digitorum brevis and the toe flexors, building grip strength in the foot that translates to better dynamic arch control during walking.
Stand on one foot for 30–60 seconds. That's it, but what's happening underneath is significant. Single leg balance forces your intrinsic muscles, ankle stabilizers, and arch musculature to work together in real time under bodyweight load. Progress by doing it on a slightly unstable surface (a folded towel or balance disc) or with eyes closed, which increases the demand on proprioception, the body's sense of its own position in space.
This is the question everyone asks, and the honest answer has some nuance.
The frequently cited statistic, that plantar fasciitis resolves within 12 months in approximately 90% of cases with conservative treatment, is accurate but incomplete. That timeline assumes consistent, appropriate treatment. It is not a passive process.
The most common mistake people make is treating the condition as resolved the moment pain decreases, then returning immediately to the same habits that caused it. Plantar fasciitis is well-known for relapse. The goal of treatment should always extend beyond pain elimination to genuine tissue resilience.
Plantar fasciitis is very manageable with self-directed treatment in most cases, but there are situations where professional assessment is the right move.
See a podiatrist, orthopedic specialist, or physical therapist if:
A proper evaluation can rule out other causes of heel pain, identify biomechanical contributors that home treatment cannot address, and open the door to interventions like orthotics, PT, and imaging that significantly accelerate recovery.
Most people do at least two of these without realizing it. Any one of them can stall progress for weeks.
1. Walking barefoot on hard floors
This is probably the single most common mistake. You do your stretches, you wear your supportive shoes outside, and then you walk barefoot across tile and hardwood all day at home. Every barefoot step on a hard surface loads the plantar fascia without any cushioning or arch support. Get a pair of supportive slides and wear them around the house. It's not glamorous advice, but it works.
2. Ignoring calf tightness
If you're stretching your plantar fascia but skipping the calf stretches, you're solving half the problem. Tight calves are one of the most consistent risk factors in the research. The tension travels directly down the kinetic chain to the heel attachment. Calf stretching is not optional. It's foundational.
3. Wearing worn-out shoes
A shoe that looks fine from the outside may have a midsole that compacted months ago. Most supportive shoes have a functional lifespan of 8–12 months under regular use. If you can't remember when you bought your current everyday shoes, that's probably your answer. Continuing to wear them is the equivalent of sleeping on a broken mattress and wondering why your back hurts.
4. Stopping exercises too early
Pain decreasing is not the same as tissue healing. People commonly stop their stretching and strengthening routine the moment they feel better, which is usually well before the tissue has fully remodeled and the intrinsic muscles have built real strength. Stopping early is one of the primary drivers of relapse. A good rule of thumb: continue your routine for at least 4–6 weeks after pain resolves.
5. Returning to activity too quickly
Runners are especially prone to this one. Pain starts improving, so they go back to full mileage. The tissue isn't ready. The cycle restarts. Returning to activity after plantar fasciitis should be gradual, ideally with a structured ramp-up plan that increases load by no more than 10% per week. If pain returns during a session, that's the tissue telling you it wasn't ready. Listen.
Plantar fasciitis is one of those conditions that tends to arrive quietly, then overstay its welcome. A little heel pain becomes a bigger heel pain. A morning wince becomes a day-long ache. Before long you're rethinking which floors you'll walk on and whether it's worth getting up at all.
But the research is consistent: this condition responds exceptionally well to the right combination of targeted stretching, strengthening, footwear improvement, and patience. Most people who treat it correctly and address the underlying causes, tight calves, weak foot muscles, unsupportive shoes, get fully better and stay better.
Start with the fundamentals. Stretch your calves and your plantar fascia daily. Wear supportive footwear, not just when you exercise, but throughout the entire day, including at home. Begin building the intrinsic foot strength that your shoes have been doing the work for. And give it time.
Your foot is a remarkable structure. It just needs the right conditions to heal.
Continue Reading:
What is plantar fasciitis?\
Plantar fasciitis is irritation and degeneration of the plantar fascia, a thick band of connective tissue that runs along the bottom of your foot from your heel to your toes. It is the most common cause of heel pain in adults and is characterized by sharp pain with the first steps in the morning or after periods of rest. In chronic cases, research increasingly points to tissue degeneration (sometimes called plantar fasciosis) rather than pure inflammation as the dominant process.
What causes plantar fasciitis?
The most common causes are repetitive stress on the plantar fascia from prolonged standing or activity, tight calf muscles that increase tension on the heel attachment, flat feet or high arches that alter how force is distributed, and footwear that fails to provide adequate support or cushioning.
Can plantar fasciitis go away on its own?
It can improve, but without addressing the underlying causes, tight calves, weak foot muscles, inadequate footwear, the condition tends to persist or recur. Consistent, targeted treatment is the difference between resolving it in 8 weeks or tolerating it for 18 months.
How long does plantar fasciitis last?
Mild cases often resolve in 6–8 weeks with proper care. Moderate cases typically take 3–6 months. Chronic cases, those present for longer than 6 months, require professional evaluation and a structured treatment approach. The majority of cases resolve within a year with appropriate treatment.
What shoes help plantar fasciitis?
Shoes with adequate arch support, firm heel counters, generous cushioning in the midsole, and a wide enough toe box to allow natural foot splay. High-drop shoes that elevate the heel can provide temporary relief, while supportive zero-drop options may be better long-term once the calf musculature is conditioned. → See Best Shoes for Plantar Fasciitis
Does walking help plantar fasciitis?
Moderate walking is generally fine and beneficial. It promotes blood flow and maintains mobility. High-volume walking on hard surfaces without proper footwear is the problem. Avoid going barefoot on hard floors, especially in the morning when the fascia is at its most vulnerable.
Can tight calves cause plantar fasciitis?
Yes, and this is one of the most underappreciated causes. Tight gastrocnemius and soleus muscles restrict ankle dorsiflexion and increase the mechanical tension transmitted to the plantar fascia through the Achilles tendon. Calf stretching is the most evidence-supported conservative treatment for this reason. → See How Tight Calves Cause Foot Pain
What is the fastest way to heal plantar fasciitis?
Consistency over cleverness. The evidence-based fast track is: daily plantar fascia stretching before your first morning step, twice-daily calf stretching, wearing supportive footwear throughout the day including at home, beginning intrinsic foot muscle exercises, and adding night splints if morning pain is severe. Starting physical therapy early in the process meaningfully shortens recovery time.
Can standing all day cause plantar fasciitis?
Absolutely. Prolonged standing, especially on hard surfaces without adequate footwear, is one of the primary risk factors. This is why healthcare workers, retail employees, and teachers are among the highest-risk populations. → See Why Your Feet Hurt After Standing All Day
Should I stretch plantar fasciitis?
Yes. Stretching is among the most effective interventions supported by clinical research. Plantar fascia-specific stretching and Achilles tendon stretching are both well-evidenced. The plantar fascia stretch performed before getting out of bed each morning is particularly effective at reducing that first-step pain.
Can plantar fasciitis cause arch pain?
Yes. While heel pain is the hallmark symptom, the plantar fascia runs the entire length of the arch from the heel to the toe bases. As irritation increases or the condition progresses, pain can radiate from the heel into the arch itself. Some people experience arch pain as their primary symptom, particularly those with flat feet or significant overpronation. If your arch pain is dominant without much heel involvement, it's worth having a clinician confirm the diagnosis, since arch-dominant presentations can sometimes overlap with other conditions.
Medical Disclaimer: This content is for educational purposes only and does not constitute medical advice. If you are experiencing persistent or worsening foot pain, consult a qualified healthcare provider.
Research References: